Donkeys are known to get a little chunky and by chunky I mean fat deposits externally and internally which are detrimental to their health and wellbeing. Further, keeping your donkey at an ideal weight is of the utmost importance for the prevention of laminitis.
Here is some nutritional information for caring for your donkey:
Feed 1.5-2% of body weight in forage per day.
Generally, once the energy (calorie) requirement has been met, their protein requirement will have also been met. Donkeys also only require about 75% of the calories that a horse of a similar weight would need which is why they are often referred to as “super keepers.”
Donkeys have rather large intestines, which they use to full capacity, and will retain forage longer to digest their intake more thoroughly. Due to their increased capacity and retention, donkeys often have a “hay belly” appearance, or an “A” frame appearance.
1. Feed roughly 75% straw and 25% hay ,except during the winter when you can feed 50/50 straw and hay.
2. Barley straw is ideal, followed by wheat straw and then oat.
3. Vitamin / Mineral supplement or Ration Balancer • Use a low sugar/starch carrier for supplements such as Timothy Pellets or Non-Molasses Beet Pulp. Ration balancing supplements with a 3- to 4-ounce serving size are typically a better choice.
4. Access to water 24/7 despite the belief that they do not need as much water as horses, they DO!
5. Avoid sugary treats.
6. Muzzle. Muzzle. Muzzle. OR Dry Lot. Once your donkey gains weight not only is it difficult to lose, the fat deposits (the fallen crest, lumps) may never go away. It is easier to be proactive than it is to be reactive. Even if the grass looks sparse, due to their “desert” ancestry, any grass is considered “lush.”
White Line Disease is extremely common in donkeys and can cause major issues if severe or left untreated.
What is White Line Disease or Seedy Toe?:
The white line is seen on the underside of the foot. It is where the unpigmented horn of the inner hoof wall joins the horn of the sole. Degeneration of the horn at the white line leads to separation of the hoof wall from the underlying structures and weakening of the hoof wall.
Risk Factors:
The reason why WLD occurs isn’t fully known, but anaerobic bacteria and fungi alongside poor foot hygiene play an important role in the development of the disease.
Some of the risk factors associated with the development of this condition are;
1. The presence of horn digesting microbes (Pseudoallscheria boydii, Scopulariopsis spp., Aspergillus spp, Fusobacterium necrophorum, penicillium spp.)
2. A wet and humid environment, poor foot hygiene, 3. Pre-existing laminitis resulting in a stretched white line 4. Hereditary factors.
Donkeys seem to be more susceptible to WLD than horses. It can affect any of the four feet and recurrence is common. Generally donkeys with WLD will not be lame, but depending on the severity of the pathology or the presence of other associated diseases, lameness could be present.
Prevention:
Maintaining good foot hygiene and regular foot care will help to prevent the occurrence of WLD. The following are best practice for prevention of this condition:
1. Clean the hooves daily, monitoring the integrity of the white line and the rest of hoof structures.
2. Change bedding frequently, avoiding humidity and accumulation of faeces and urine, especially in wet seasons.
3. Arrange for your farrier to check and trim the feet every six to ten weeks depending on the amount of exercise/wear, the age of the donkey and/or the presence of hoof pathology.
4. Avoid grease or similar products as they reduce horn oxygenation and can create an environment that encourages proliferation of horn digesting microbes.
5. Monitor animals with a history of WLD closely as they will be more susceptible to recurrence.
6. Good, clean hard standing and dry bedding are important for the health of all donkeys’ feet, but for animals with recurrent WLD it is very important.
Treatment Options:
1. Resection: Your farrier or vet will remove all the damaged horn. This procedure should not be painful but it may be necessary to remove a lot of hoof wall if the disease has progressed. In some circumstances it may be necessary to take an x-ray before removing a large amount of hoof wall to check the stability of the pedal bone.
2. Cleaning and Medicine: Once all the damaged horn has been removed, the hoof needs to be kept clean with daily hoof picking and brushing to remove as much organic matter as possible. Once the foot is clean topical disinfectants (eg povidone iodine, hydrogen peroxide or zinc sulfate) in solutions or sprays are useful to reduce microbial contamination.
3. Other Treatments: Removing all the abnormal horn, ensuring good oxygenation to the area and maintaining good foot hygiene may be enough to manage the problem. However, if the amount of wall that has been removed is substantial, your vet or farrier may decide to refill the defect with acrylic material to give more stability to the hoof capsule. In these cases it is vital that all the affected horn is removed to ensure the acrylic material bonds to healthy horn.
Sweet Vera was acting lethargic one evening. She did not show any obvious signs of colic like pawing or distress. However, she was laying down more than typical. Whenever approached she would stand up. The most obvious sign was that when she was offered a treat she was not interested. I took her temperature and it was normal. Gut sounds were present but she looked bloated. I decided to give the vet a call. The vet came and tubed her and gave her some banamine. When Vera was tubed, but due to her small stature, a smaller tube had to be used and not much came out.
The next day she continued to act off. Again, I called the vet and decided to bring her into the hospital. There the vet tubed her at intervals throughout the day and into the next. They gave her fluids via an IV and did a few ultrasounds . Thankfully they were able to get a larger tube in her and the thick, paste like substance started coming out…more and more and more. The interesting part of this was that she does not get grain. There was no sand in the substance that was removed from her belly but my guess is someone gave her treats and due to the extreme heat she was not drinking as much- basically, a perfect storm hit.
Day three she began to perk up, have bowel movements, and even started eating some mash. The next day she was able to return home and has been doing well.
How to Spot Colic in Donkeys?
Dullness
Lying down
Lack of appetite or refusing to eat
Weight shifting, usually between the hind legs
Rolling and pawing at the ground (rare in donkeys, can indicate a serious problem)
Fast breathing, rapid heart rate
Sweating
Brick red or pale gums or insides of eyelids
Dry or tacky gums
Lack of, or reduction in, the normal quantity of droppings
Self-isolating or moving away from companions.
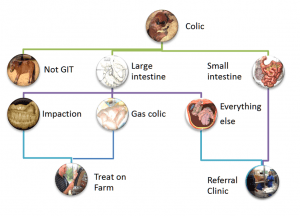
Types of Colic:
Impaction Colic: Impaction occurs when forage, sand, dirt or other material gets lodged in the colon, causing the horse to be unable to pass manure and putting a halt to the whole digestive system. Impaction can also be caused in some cases by enteroliths, naturally occurring mineral deposits that can reach up to 15 pounds in size. Impaction colic tends to occur more in the winter months, due to a lack of hydration.
Gas Colic: Gas colic is a mild, abdominal pain stemming from the result of gas buildup in the horse. This can be caused by a change in diet, low roughage consumption, parasites or administration of wormer.
Sand Colic: Sand colic is caused by the abnormal consumption of large amounts of sand while grazing or eating off dry, sandy ground. Upward of 80 pounds of sand have been found in a colicking horse’s gut. Naturally, sand colic is more common in southern regions where the ground tends to be more mineralized. One way you can help prevent sand colic is to avoid feeding horses from the ground, and instead use a feed pan, bucket or feeder.
Entrapment (or Displacement) Colic: Displacement transpires when the large colon moves to an abnormal location, often occurring at the pelvic flexure, an area where the colon narrows and makes a sharp turn. In some cases, displacement can also lead to entrapment, where something traps the gut and can cut off blood supply.
Enteritis: Abdominal pain can also be caused by enteritis, the general inflammation of the gut. This inflammation is most commonly caused by colonization of the gut by pathogens (bacteria or viruses). Learn more about this in the Importance a Balanced Gut Microbe Ratio in the Gut.
Strangulation (or Gut Torsion or Twisting) Colic: A twist occurring in the gut causes strangulation colic, which often cuts off blood supply and results in dying tissue. This type of colic is very serious and the most likely to be fatal.
Enterolith: Enteroliths are mineral accumulations of magnesium-ammonium-phosphate (struvite) around a foreign object (a piece of metal, pebble, bailing twine, hair, rubber) that form round, triangular, or flat stones inside the bowel usually over the course of multiple years. They form in the large colon of horses where they can remain for some time until they move and cause an obstruction in the large or small colon, resulting in colic.
Idiopathic or Spasmodic Colic: The majority of colic cases are idiopathic. This means the cause is unknown or unable to be determined. This is a wide-ranging term for horses presenting with colic where other abnormalities cannot be found, and, which generally have increased gut movement (and therefore gut noise if you listen over the belly). The colic signs are associated with increased gut spasm due to the increase in motility (a horse equivalent to gut cramps that we may experience after a very spicy curry for example). Rectal examination is within normal limits in these cases and, these horses often respond very favorably to drugs that decrease gut motility (see treatment of colic).
Treatment Options:
Your vet may carry out the following to try to diagnose the type of colic:
Checking your donkey’s heart rate and temperature.
Listening to your donkey’s abdomen with a stethoscope to check the gut sounds
Checking your donkey’s teeth
Taking a blood sample
Performing a rectal examination
Passing a stomach (nasogastric) tube to check for reflux (backed up food or fluid). Your vet will decide on the best treatment based on your donkey’s diagnosis and are likely to give painkillers.
Depending on their findings, your vet may give your donkey fluids via a nasogastric tube or put them on a ‘drip’ (usually via the large vein in their neck). It may take multiple visits from your vet to treat your donkeys colic.
Your donkey may need to be hospitalised if their case is severe. If your donkey is hospitalised, their companion must go too, as hospitalisation can be very stressful for donkeys. Some types of colic need surgery to resolve them, which will require prompt transport to a hospital. Surgery carries a high risk in most colic cases and involves considerable nursing care and cost. Check you are insured for the costs and talk to your vet about the chances of success.
Euthanasia may be the kindest option if your donkey’s case is serious.
Prevention:
Colic is so dangerous because by the time your donkey lets you know it has colic, it may be too late to save it. The old adage, ‘prevention is better than cure’, definitely applies.
Observe your donkey daily, looking for any changes in behaviour. Know what typical dung looks like. Be aware of the average number of piles of droppings your donkeys pass each day and the consistency. Persistently very loose or very dry droppings could be indicative of colic, particularly if other symptoms appear. Check your donkey’s breathing pattern so you will be able to spot any change.
Colic Causes & Prevention:
Feed – sudden changes to diet, poor quality feed, too much grass, feeding cereals:
Make any dietary changes gradually over at least a week, ideally 2-4 weeks
Feed good quality forage and donkey specific proprietary feeds
Avoid moldy feed
Always soak sugar beet to the manufacturer’s recommendations
Feed little and often, especially if your donkey has additional feed
Do not allow your donkey access to too much rich spring grass.
Inadequate or dirty water supply:
Check troughs daily. Self-filling drinkers can become blocked, or the water supply can fail
Clean dirty water containers as donkeys will not drink dirty water
Check water is not frozen or too cold. Many donkeys will not drink very cold water
Offer several sources of water.
Eating non-food items such as plastic bags, rope or bedding:
Ensure your donkeys cannot access non-food items
Change your donkey’s bedding to something less palatable, such as wood shavings
Do not use cardboard or paper bedding.
Eating poisonous plants:
Know your poisonous plants and trees
Remove poisonous plants or fence off the problem area
Check pasture, boundary fences and hedgerows frequently
Fence off trees when fruiting to prevent your donkey gorging.
Sandy soil:
Avoid grazing on sandy soil pasture if possible.
Dental disease – failure to chew food adequately resulting in a blockage of the gut:
Have your donkey’s teeth checked at least annually by a qualified equine dental technician or vet
Dental disease is more common in older donkeys
Suspect dental problems if donkeys are ‘quidding’ (dropping part chewed feed) or drooling saliva
Parasites – worms causing obstruction or inflammation of the gut:
Arrange regular faecal worm egg counts to check if your donkey needs treating for worms
Speak to your vet for advice
Clear droppings from your donkey’s paddock at least twice a week.
Stomach ulcers:
Keep stress to a minimum
Trickle feed your donkey.
Pain – any painful condition can lead to colic, including severe lameness:
Ensure your donkey has adequate pain relief if they have a painful condition.
So, I wish I did not have to start this process again…but unfortunately, I do. Once again I have a senior horse with a variety of acute and chronic conditions that all hit at the same time. Right now I am trying to make her comfortable while also trying to figure out what is what and how to best respond.
Three months ago Tilly was tested for EPM due to muscle wasting and weight loss.The first time she was in the lower end of an active infection. We started a compounded medicine for 1 month and her numbers decreased. We decided to do another round as she responded well to the first round. However, the numbers remained the same. We also tested her for Lyme which showed a chronic and an active infection but the numbers were in the high normal range and the vet felt that it was not treatment worthy at the time.
Last month Tilly began “crab walking” out of the blue. Called the vet. They came out. Her ataxia was bilateral- both her left and right hind- whereas EPM tends to be unilateral. Further, her presentation was not suggestive of Lyme.
We started steroids (dexamethasone oral power) for 5 days with Banamine, tapering as we went, and she seemed to recover. The consensus was it was an acute attack that may have occurred given she is a senior with a history of being an Amish workhorse and perhaps, she pulled something in her neck.
Treatment was complete and another week went by and again, she showed some ataxia. This time less severe. The vet felt that since she responded well to the first round of steroids that it was not EPM-related as you would not see improvement. Further, if it were Lyme related the presentation would be more consistent. Again, a round of Dex and improved quickly. The next week we had her neck x-rayed and there were some arthritic changes. However, she was running around and moving well so the vet felt injections in her neck would not be necessary at that time.
Seventy two hours later, she had some trouble getting up but eventually succeeded. The next morning my sweet girl was spinning, crab walking, and falling over. It was absolutely terrible to see. I immediately gave her 10cc IV Banamine and she calmed down and stopped spinning. The vet came out and administered Dex IV and thought that due to her inflammatory bowel disease we should try Dex IM to ensure absorption. We also decided to pull blood to test for Cushings as she seemed to lose weight overnight and was not shedding out well. The next day she was lame on her right front. Panicked I called the vet fearing that if she did have Cushings, she was trying to founder due to the steroid use. Thankfully, the vet came out, did a nerve block on her right front (this helps to see if the horse has laminitis as they will improve once blocked) and checked for pulses (if a horse has laminitis typically they will have pulses in their hooves) and Tilly did not have any. So, the vet did not feel we were dealing with founder. However, the lameness presented a major challenge due to her still being ataxic on the hind end. The vet did cortisone injections into her neck hoping to help with inflammation due to arthritis. Tilly did great and suddenly, began freaking out. Spinning, knocking into the doors, etc. The vet explained that the injections likely added more pressure on her spinal cord causing her to react. Again, once the vet was able to safely administer Banamine and some Dorm, she calmed and laid down for the first time in over a week for a good 45 minutes. We decided to make sure she was able to get back up. Although she had some trouble, after a couple tries, she was able to do so. Her breathing was heavy, wheezy, almost like she was having a panic attack and hyperventilating. A few minutes later, her breathing returned to normal.
Tilly’s Cushing’s text level was about 100 pg/mL (it should be about 30 pg/mL during mid-November to mid-July) meaning, she does have Cushings. The vet decided to wean her off of the steroid as to not increase the risk of Laminitis even more but also to give neck injections time to work (5-7 days). We also immediately began Prescend (2 tabs) a day to treat her Cushings.
We are on day 5 since the 3rd ataxic episode and day 3 post neck injection and she is still lame on her right front along with ataxic on her hind end. However, she is still eating, engaging, and is bright and alert. She does not seemed distressed or in pain thankfully. Due to Tilly not showing much improvement (even though it can take 5-7 days to see improvements from the neck injections) I decided to start her on a non-compounded EPM medication, Protazil. According to the vet, Protazil should not cause any harm whether her symptoms are EMP related or not. I also began 10cc of Vitamin E oil. Tilly was previously on pelleted Vitamin E but due to her inflammatory bowel disorder, she may struggle to absorb the pelleted form of the supplement. Further, there are a number of studies showing the benefits of Vitamin E and the connection between Vitamin E and ataxia.
On a positive note, since starting Prescend for her Cushings, I have noticed that she is drinking less water. Increased water intake is a symptom of unmanaged Cushings. I am hopeful that means the medication has started to work at regulating her hormones. We are now at a wait and see point. I continue to try to make her comfortable. Tons of bedding in her huge foaling stall, hay everywhere, fans on, doors open. She has been a trooper. My hope is that she recovers from this and enjoy whatever time she has left and fights this as she has so many other things- the reason she was given the name, Ottilie.
My senior Belgian Draft mare has a chronic condition where her stools are relatively solid but after having a stool, she passes fecal liquid separately, Her tail and hind end, and legs are covered. Initially when she came to me she had loose stools and the vet did a fecal and we put her on Biosponge. Her Fecal Sample showed minimal infestation and the Biosponge did not do much. Over time, her stools became more solid but the liquid continued. Now, after being with me for about 6 months we are still having this issue.
So, I did some research and came across an article on something I had never heard of before- Fecal Water Syndrome. According to an article on SmartPak.com, Fecal Water Syndrome is typically caused by the following;
The underlying cause of FWS in horses is not known at this time and there are many theories as to why some horses develop it. A group of researchers in Germany set out to explore some of the proposed theories and discovered that neither dental disease nor a heavy parasite burden seemed to be associated with FWS. However, it was found to be more likely to occur:
in horses of low rank or “pecking order” in the social hierarchy of a herd
in winter when subordinate horses were confined to a smaller space, leading to anxiety
in geldings vs mares, which are usually more dominant than geldings
in paint horses
However, the article also noted that due to FWS being a relatively new diagnosis, more studies are needed to look at the role stress, nutrition, and potentially, other factors in the development and management of FWS.
Diagnosis of FWS
Most veterinarians approach the diagnosis of a horse with FWS similar to one with diarrhea or loose stool. That is, they start by taking a thorough history from the owner, then perform a complete physical examination with special emphasis on the digestive system, and finally may recommend specific tests to evaluate the health of the horse in general and the GI tract in particular. It can be helpful to confirm the presence of soiled hind limbs and tail as well as dirty stall walls and bedding. While on the farm, the vet may want to walk through the regular feeding and management programs including turnout and herd status.
Treatment and Management of FWS
Although there is no standard treatment or set of recommendations for the care and feeding of horse suffering from FWS, all potential causes for disruption in the GI system should be addressed, including social stress.
Making adjustments to the horse’s turn-out time and group.
Making adjustments to the diet (with the input of a veterinarian and nutritionist.)
Trying out various medications and supplements one at a time on the passage of fecal water. For example, adding omega 3 fatty acids for a normal inflammatory response in the gut, and to the stabilizing effects of “baker’s yeast” or Saccharomyces cerevisiae.
Make sure to keep the hindquarters clean and dry to prevent any sores for forming.
Equine First Aid Kit All horse owners should have an equine first aid kit & know how to use all of the supplies. At least twice yearly, examine & replenish outdated supplies. Store your first aid kit in your home or temperature controlled space. Leaving it in a trailer or uninsulated tack room will quickly degrade the supplies. Talk to your veterinarian about customizing your first-aid kit for your horse’s particular needs.
FUNDAMENTALS Thermometer, Mercury or Digital Stethoscope (good quality) Headlight (good quality) Proper Fitting Halter & Lead Rope Latex Gloves (12) Watch or Timepiece with Second Hand BASIC EQUIPMENT Bandage Scissors Suture Scissors Tweezers or Forceps (smooth jaws) Non-Sterile Gauze – 4″x4″ Squares (1 package) Conform® or Kling® Gauze 4″ (2 rolls) Elastic Adhesive Bandage (Elasticon®) 3″ (2 rolls) Cohesive Bandage (Vetrap®) 4″ (2 rolls) Non-Adhesive Wound Dressing (Telfa® pads) 3″x4″ (2) & 3″x8″ (2) Povidone Iodine (Betadine®) Solution (4 oz) Antiseptic Scrub, Chlorhexidine or Povidone Iodine (Betadine®) Scrub (4 oz) Sugardine Small Plastic Containers for Mixing or Storage (2) Wound Lavage or Cleaning Bottle, Saline (250 ml) Tongue Depressors (6) Alcohol Wipes (10) Spray Bottle for Water (1) Paper Towels (1 roll) Multi-Purpose Tool, Leatherman® or Equivalent Cotton Lead Rope (3/4″ – 1″ in diameter) Electrolytes (paste or powder) Fly Repellent Ointment (1) Heavy Plastic Bags (2 – gallon & 2 – pint size)
SECONDARY EQUIPMENT Cotton, Rolled Sheets, Leg Cottons (2) Standing Wrap & Quilt or Shipping Boots Easy Boot or Equivalent in Appropriate Size Baby Diapers (2) (size 4 to 6 depending on hoof size) Triple Antibiotic Ointment (1 tube) Extra Halter & Lead Rope Lariat Syringe 35 cc (1) Syringe 12cc (3) Syringe 3 cc (3) Syringe 3cc with 20gauge needle (3) Syringe – 60 cc cath tip (2) Needles – 18gauge – x 1.5″ (4) Needles – 20 gauge – x1.5″ (4) Eye Wash, Saline (1 bottle) Opthalmic Ointment or Drops (1 bottle or tube) Magnesium Sulfate, Epsom Salts (1 package) Duct Tape (1 roll) Clippers with #40 Blade (good quality) Shoe Puller Crease Nail Puller Hoof Pick Hoof Knife Hoof File, Rasp Clinch Cutters Farrier’s Driving Hammer Collapsible Water Bucket Ice Wraps Twitch Bute Banamine Bordered
Talk to your veterinarian about dispensing a few medicines that you may use in an emergency. In most, if not all states, a veterinarian cannot legally dispense prescription items without a valid Veterinary Client Patient Relationship (VCPR).
• Flunixin Meglumine (Banamine®) (injectable or paste) • Phenylbutazone, Bute Paste (1) • Trimethoprim-Sulfa Tablets SMZ-TMP in small container (75#)
Tilly came to me from a slaughter auction in Texas after 17-ish years as an Amish workhorse. She was thin (she still is), sick (upper respiratory infection) had cracked hooves, had never had her teeth floated (they made a horrible grinding and clicking sound when she ate), and apparently had never been clipped or bathed or worn a blanket. I do not think she had ever even had a treat (she still won’t take an apple or carrot).
SYMPTOMS:
Rumbling gut
Cow pie stools
Grinding/clicking teeth
Cracked hooves
Dull coat
Underweight
Running nose
PROFESSIONALS:
Farrier for evaluation and trimming
Dentist for power float of teeth
Vet for physical, blood work, and fecal
TESTING/RESULTS:
CBC: all in normal range aside from her creatinine and protein suggesting dehydration. These values normalized after about 1 week)
Fecal: Minimal
FEED:
Triple Crown Senior Feed (Low sugars, low starch, high fat)
Tons of water with Horse Quencher added
Salt block
MEDICATIONS:
Exceed injections (2 total a week apart) then SMZ for 2 weeks
Banamine
Brewer’s Yeast (Stomach)
BioSponge (Gut health and to tackle her loose stools)