

Category Archives: Misc Equine Topics
The Leader of the Pack
When meeting new friends it is important to show that you maybe 32 years old but you’ve still got it…even if that means being sore the next day!




Home is Whereever You Are
Recently, I had to move to a new farm. And, if you are anything like me you loathe not only moving but moving your horse. The what-ifs running though my head- what if he won’t load? What if he hits his head? What if he freaks out? (Or to be completely transparent, what if I do?). What if he falls? Etc. Personally, when I am faced with a anxiety provoking situation, I need to have a sense of control however small it is. So, I did what I do best and planned and organized. Everything.
Chance had a bad prior experience with being trailered. Plus, with his age (31) and past health issues my anxiety was at an all time high. It was recommended that I plan to meet him at the new farm instead of being there for loading. Made sense. I scheduled the vet to be there in case medications were needed. And they scheduled a therapeutic trailering service with a large trailer that had an forward unloading ramp. The horse communicator was also scheduled as she knew of Chance’s past experience and did energy work.
The day arrived. I went to the farm early and wrapped Chance’s legs, brought he and Lucky inside, packed up all my stuff, and met with the horse communicator. She did some grounding exercises with Chance and myself. I left when everyone arrived and went to the new farm and unloaded our stuff. About 1 hour later the phone rang and of course, I thought the worse. Chance refused to load even after 2 rounds of medications. Lucky was on the trailer. They requested I come and try. I drove the 30 minutes back to the farm- praying to everyone and anything- that Chance would load. I read some tips on Google (yes, I’m ashamed to admit, while driving). One article suggested doing groundwork to get the horse to pay attention. For example, stop him, make him stand, back up, etc. Once he was listening that is when you try to load. The article went on to say that anger and frustration would not work. Because a horse is in sync with our emotions. And that physically, a horse has stamina that we as humans do not share. However, mentally the horse will give up quicker. Patience. Kindness. Persistence.
I arrived. I followed the advice of the article. I walked him and gave commands. I was cool, collected, firm, and kind. We tried once. He walked part way up the ramp, stopped, and backed up. Again, I did the commands. Tried once more. Same thing. The third time the lady who was there to Trailer him lightly smacked his butt with a crop and suddenly, he was on the trailer! I couldn’t believe it. We quickly shut the doors and off we went.
The trip was about 45 minutes. And, thankfully, uneventful. The trailering company was amazing and patient. I’m beyond grateful for everyone’s help!
Below is information for trailering issues, how-tos, and professionals that can make the transition 10000% easier and, almost, stress free.
Resources:
1. True North Equine in Marshall, Virginia
2. Trailering service: Always There Horsecare: 703-915-6255 or http://www.alwaystherehorsecare.com
3. Article: Think like a horse
4. Article: The hard to load horse
5. Article: Lets Get Loaded



Science: When Horses Are in Trouble They Ask Humans for Help, Finds New Study
Research Fellow Monamie Ringhofer and Associate Professor Shinya Yamamoto (Kobe University Graduate School of Intercultural Studies) have proved that when horses face unsolvable problems they use visual and tactile signals to get human attention and ask for help.
The study also suggests that horses alter their communicative behavior based on humans’ knowledge of the situation. These findings were published in the online version of Animal Cognition on November 24.
Communicating with other individuals in order to get information about foraging sites and predators is a valuable survival skill. Chimpanzees, who are evolutionarily close to humans, are especially skilled at understanding others. Studies suggest that chimpanzees distinguish the attentional states of other individuals (seeing or not seeing), and they are also able to understand others’ knowledge states (knowing or not knowing).
Some domestic animals are also very good at communicating with humans—recent studies of dogs have revealed that they are excellent at understanding various human gestures and expressions. It is thought that these abilities were influenced by the domestication process.
Since they were domesticated 6000 years ago, horses have contributed to human society in various shapes and forms, from transport to companionship. Horse-riding has recently drawn attention for its positive effects on our physical and mental health. The high social cognitive skills of horses towards humans might partially explain why humans and horses have a collaborative relationship today. However, the scientific evidence for this ability is still scarce.
In this study, scientists investigated horses’ social cognitive skills with humans in a problem-solving situation where food was hidden in a place accessible only to humans. The experiment was carried out in a paddock belonging to the equestrian club at Kobe University, where eight horses from the club participated with the cooperation of their student caretakers.
For the first experiment, an assistant experimenter hid food (carrots) in a bucket that the horse could not reach. The researchers observed whether and how the horse sent signals to the caretaker when the caretaker (unaware of the situation) arrived. The horse stayed near the caretaker and looked at, touched, and pushed the caretaker. These behaviors occurred over a significantly longer period compared to cases when they carried out the experiment without hiding the food.
The results showed that when horses cannot solve problems by themselves they send signals to humans both visually (looking) and physically (touching and pushing).
Building on these results, for the second experiment they tested whether the horses’ behavior changed based on the caretakers’ knowledge of the hidden food. If the caretaker hadn’t watched the food being hidden, the horses gave more signals, demonstrating that horses can change their behavior in response to the knowledge levels of humans.
These two experiments revealed some behaviors used by horses to communicate demands to humans. They also suggest that horses possess high cognitive skills that enable them to flexibly alter their behavior towards humans according to humans’ knowledge state. This high social cognitive ability may have been acquired during the domestication process.
In order to identify the characteristic that enables horses to form close bonds with humans, in future research the team aims to compare communication between horses, as well as looking more closely at the social cognitive ability of horses in their communication with humans.
By deepening our understanding of the cognitive abilities held by species who have close relationships with humans, and making comparisons with the cognitive abilities of species such as primates who are evolutionarily close to humans, we can investigate the development of unique communication traits in domesticated animals.
This is connected to the influence of domestication on the cognitive ability of animals, and can potentially provide valuable information for realizing stronger bonds between humans and animals.
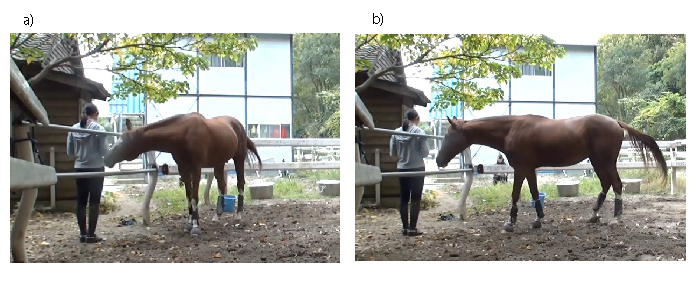
Figure 1. Horse making demands: The horse a) lightly pushes and b) looks at the caretaker standing outside the paddock. Food is hidden inside one of the two silver buckets behind them. When horses cannot obtain this food by themselves, they give humans visual and tactile signals.

Photo provided by Monamie Ringhofer.
Figure 2. Horse with caretaker at the equestrian club

The Heart of the Matter


I Loathe Ticks!
Your horse comes in from being outside and is barely able to move. His legs are swollen, he has a fever, is sensitive to the touch, and has a loss of appetite. He has chills- intermittently shaking. He wont touch his hay, his eyes are dull, and he looks depressed and tired. You call the vet and they run hundreds of dollars worth of tests- CBC, x-ray his legs to ensure there is no fracture; they diagnose him with Lymphingitis. You begin a course of antibiotics. You cold hose. You give him Banamine. Your wrap his legs while he is on stall rest. A week later, the swelling has subsided, his fever has dissipated, and his appetite is back.
You get a text saying that your horse “ran away” when he had been let out earlier that day. But when you get to the barn, you notice when he turns he looks like his hind end is falling out from under him..remember when you were little and someone would kick into the back of your knees and your legs would buckle? That is what it looks like. So you watch him. You are holding your breath, hoping he is just weak from stall rest. You decide, based on the vet’s recommendation, to let him stay outside for the evening. You take extra measures- leaving his stall open, with the light on, wrapping his legs, etc- and go home. Every time your mind goes to “what if..”, you reassure yourself that your horse is going to be okay and that you’re following the vet’s advice and after all, your horse had been running around earlier that day.
The next morning your horse comes inside and it takes him an hour to walk from the paddock to his stall. All four legs are swollen. He has a fever (101.5). He is covered in sweat. He won’t touch his food. He has scrapes all over his body and looks like he fell. You call the vet- again- and they come out to look at him. They note his back sensitivity, his fever, the swelling at his joints (especially the front). They note that his Lymphingitis seems to have come back. The vet draws blood to check for Lyme. They start him on SMZs and Prevacox. You once again wrap his legs, ice his joints, give him a sponge bath with alcohol and cool water to bring down his fever. You brush him, change his water, put extra fans directed at his stall. You put down extra shavings. And you watch him.
A few days go by and you get a call saying that your horse has tested positive for Lyme…and while your heart sinks, you are also relieved that there is an explanation for your horse’s recent symptoms. You plan to begin antibiotics and pretty much not breathe for the next 30+ days while your horse is pumped with antibiotics. You pray that he doesn’t colic. You pray that you have caught Lymes in time. You pray that the damage is reversible. You research everything you can on the disease. And you sit and wait….
Below are resources on Lyme Disease in horses- treatments, symptoms, the course of the disease, and the prognosis.

Lyme Disease in Horses | TheHorse.com
Lyme Disease, testing and treatment considerations | Best Horse Practices
Microsoft Word – Lyme Multiplex testing for horses at Cornell_2-12-14 –

Fall Fever
Today Chance had swelling of his back right fetlock. He had a fever around 104 and didn’t eat his feed. His eyes were dull and he was lethargic. He wasn’t limping but was walking slower than normal (he usually runs to the paddock or back to the barn). I decided, due to the Lymphingitis flare up on his back right leg, I would give him a shot of 5 mls (or 5 cc) of Banamine and wrap his leg. Once the medication set in, I would bring him in to give him a bath (it was 80 degrees today). So, that is what I did. By the time he was back at the barn he was covered in sweat. I cold hosed him and drenched the wrap in cool water and let him roam around the barn.
Thankfully, the vet was able to meet me at her veterinary practice so that I could pick up Baytril and more Banamine. Since Chance just had Lyme Disease (and had finished his medication less than a week ago), we are not 100% if this is a Lyme reaction or something else. The plan is to administer 25 cc of Baytril either orally, in his feed, or via IV for 6 days and Banamine 10 mls (or a 1000 lbs) twice a day for 3 days. The vet suggested that I do 5 cc of Banamine if his fever remains between 101-103 degrees and 10 cc if his fever is 103 degrees or above. During this time I will begin Prevacox- one 1/4 of a tablet once a day. After 3 days, I will discontinue the Banamine and continue the Prevacox. If his fevers are not down in two days, I will continue the Baytril but start the doxycycline as it maybe a Lyme disease symptom.
While researching Lyme Disease, I found that many people do two+ months of doxycycline instead of 30 days to ensure the disease has been erraticated completely. However, since Chance had shown such improvement after 30 days, I decided to not do another month. Maybe I should have…
However, Chance had similar symptoms when we found a small laceration in the DDFT tendon of his back left hind- swelling, Lymphingitis, fever, lethargy, no appetite, etc. If he does have an issue with his tendon I will most likely do another round of Stem Cell treatments which proved to be helpful last time. Thankfully I stored his stem cells in a Stem Cell Bank (via Vet-Stem) and can easily have them shipped.

Recommended Equine Professionals and Services
True North Equine Vets www.truenorthequinevets.com 540-364-9111
Genesis Farriers: Dave Giza www.genesisfarriers.com 571-921-5822
Ken Pankow www.horsedentistvirginia.com 540-675-3815
Full Circle Equine www.fullcircleequine.com 540-937-1754
Farriers Depot: (Farrier related supplies) www.farriersdepot.com 352-840-0106
StemVet (Stem cell acquisition and storage) www.vet-stem.com
SmartPak Equine Supplements www.smartpakequine.com
|
|
|
|
|
|
|
|
|
|
||
|
|
||
|
|
||
When You Lose Your Partner
Stories from the Heart
When You Lose Your Partner

We all know the too-familiar story used in crime shows on television. A dynamic duo, perfectly paired in every way. They’re best friends who bicker like an old married couple and complete each other’s lives. That partnership is something most people long for. And it’s something a few equestrians are lucky enough to find with their four-legged half.
I was one of those few. His name was Beau. He was an off-the-track thoroughbred with a heart of gold and the chest of a draft horse. Tall, dark, handsome, loyal, always in tune with my thoughts—he was the best partner a girl could ask for.
We spent hours, days, weeks, months, training together. Athletically, we were on point. Emotionally, we were more in tune than most married couples. In every way, he was my other half. My confidence stemmed from him, and vice versa. There was nothing we couldn’t do when we were together. We literally climbed mountains.
Then, too soon, Beau passed away.

It was sudden. Unexpected. One day he was there, the next I had to make the decision to have him euthanized at the age of seven. That day I lost not only my partner, but a part of myself.
Saying goodbye to a partner is hard. For a while, there’s a hole. It never really gets filled. You keep riding, keep hopping up in that worn-out leather saddle that still smells like him. But it’s never the same. That same passion, love and commitment you shared for one another will never be replaced.
That’s a hard thing to get over. But it’s something every single equestrian will one day have to face. I hope none of you need to face it so soon. I hope your partners grow to be old and gray and pass in the most dignified and peaceful sense. I hope you have time to sit on the ground with them, no matter how hard it may be, hold their head in your lap for the last time and say goodbye.
I hope you get the chance to tell them thank you for the heart they gave you. For the confidence, experience, and love they shared with you every time you stepped into their world. But most of all, I hope you appreciate every single ride.
Go out to your barn and hug your horse.
Let them have that extra snack. Next time they decide they aren’t going to listen, or kick up their heels because they feel fresh, laugh it off. Someday you’ll miss it. You’ll miss the green stains on your white shirt from their grassy kisses. You’re going to miss braiding that mane until your arms ache. You’ll miss hitting the dirt because you couldn’t quite sit their power over that jump. Enjoy every moment of your partnership.

For those who have experienced this and said goodbye, I feel your pain. Don’t be afraid of feeling it, too. Sometimes it’s good to sit down and look at all those old photos and have a good cry over the life you had with your best friend. It’s okay for it to hurt a little bit every time you walk in the barn and they aren’t there waiting for you.
Just remember, they gave the best years of their life to you. They loved you with every ounce of their being. And you returned the favor.
About the Author
Megan Stephens is small-town equestrian from the hills of New York. She first hit the saddle at the age of four and the obsession has grown ever since. She is mom to a Hackney gelding and competes in hunter/jumper divisions for a local farm. She enjoys freelance writing about her favorite topic in her spare time.
Interviews & Profiles
Q&A: Artist Whitney Anderson Is Bringing Horses to High Fashion
Whitney Anderson was born in Alaska into a third-generation commercial fishing family and grew up in Breckenridge, Colorado, and Seattle, Washington. In 2009, she received a B.A. of…
6 days ago

Opinion
And the Sun Does Rise
It is over. Mostly. Well, except for the part about the ‘winning side’ gloating for the next year about how they were so right, and…
6 days ago

Racing
California Chrome Headed to Stud in 2017
California Chrome is heading to stud in 2017 and will stand for a fee of $40,000, Taylor Made Farm’s Duncan Taylor announced on Tuesday. The…
6 days ago

Life
The Beauty of Pony Club’s Biggest Flaw
The first six months of my riding career were spent with two trainers; one for two months, and the second for about four. Then I…
6 days ago

Uncategorized
8 Signs Your Trainer Has Adopted You
Every horse person knows the trainer/rider relationship is a little different than most coach/player relationships… About the Author Kim Ablon Whitney is a USEF ‘R’…
6 days ago

EPM Tilter. What Do The Numbers Mean?
During my horse’s recent Lymphingitis flare-up, the vet advised that we run labs to test for Lyme and EPM due to his presenting symptoms (hind weakness, twisting his back leg at the walk/walking sideways I refer to it as- “Chance’s swagger”). As I noted previously, Chance’s Lyme test revealed that he was at the beginning stages of an acute infection…yay for the labs at Cornell University for their amazing ability to give you more than a positive or negative!
A little history before getting to the EPM Tilter results.
About 2ish years ago, Chance was diagnosed with EPM (and one of the reasons opossums and I are not friends since they host the disease as do a few other culprits). Chance immediately began EPM treatment- he received Protazil in his feed for one month. After hours of research I chose Protazil, although extremely expensive (if you order from http://www.drfosterandsmith.com they sometimes have promotions where you receive store credit for every $100.00 you spend…they did when I ordered and I got a “free” dog bed that my dogs adore), due to the decreased likelihood of Chance experiencing a “Treatment Crisis” (worsening of symptoms) and the ease of administration (other brands require the drug being administered 1 hour before eating or an hour after and so on). Typically, EPM treatment is done for 30 days and, depending on the residual symptoms, some may require subsequent treatments. While Chance’s symptoms improved, I wanted to ensure that we annihilated the disease and did another round of treatment but this time with Marquis. At the end of two months, Chance’s ataxia was gone!
Fast forward to September 2016…Chance, just having a Lymphingitis flare-up, has been tested for Lyme and EPM. Lyme came back positive. And….so did the EPM test..well, kind of. Wonderful. (See why I loathe opossums?)
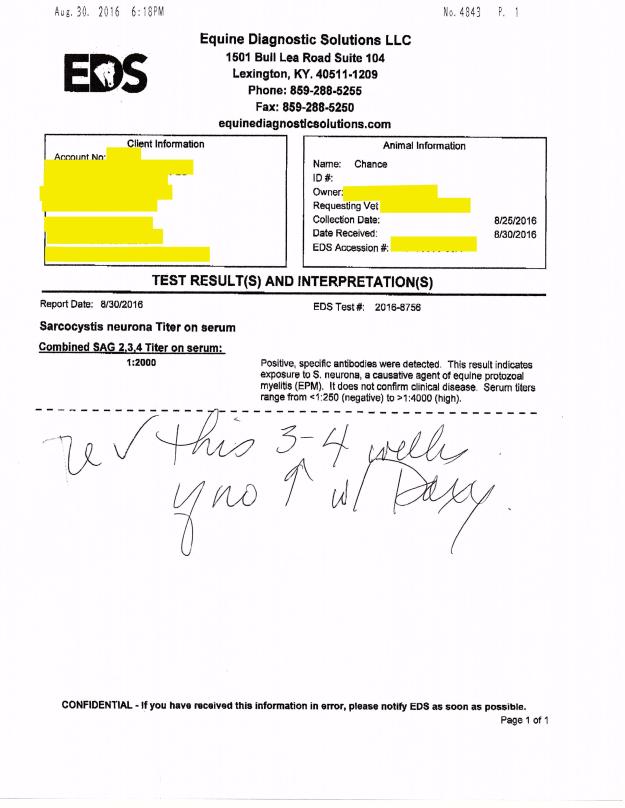
Chance’s EPM test #2 on 8/30/16 (the 1st one was 2ish years ago) showed the following:
“Combined SAG 2,3,4 Tilter on serum= 1:2000”
So, what does this mean?
The test revealed that Chance had “positive, specific antibodies” detected in the blood work. This means that he had EXPOSURE to S. Neurona, a causative agent of EPM. Serum tilters range from <1:250 (negative) to >1:4000 (high positive). S. Neurona (SarcoFluor) is one of two protozoa found in EPM infected horses, the other protazoa is N. Hughesil (NeoFluor). S. Neurona is most frequently seen, whereas N. Hughesil is not as common.
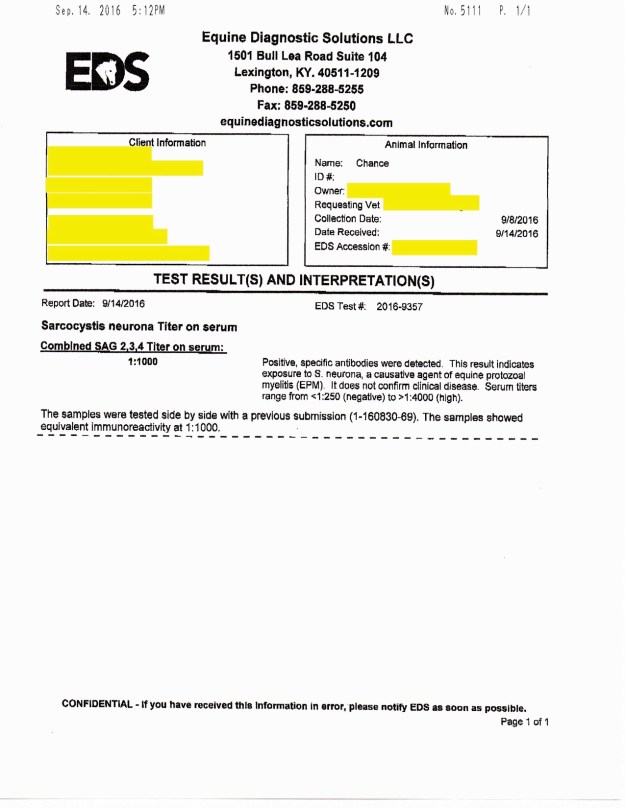
The vet ran another EPM test to confirm the findings in the 8/30/16 test. The results showed that Chance had “Combined SAG 2,3,4 Tilter on serum= 1:1000. Again, Chance showed EPM protozoa in the positive-ish range.
I initially had not seen the results but was told by the vet that he was EPM negative. So when I asked for the test results to be emailed to me and saw the numbers I sort of freaked out…I emailed the vet to ask for clarification. She explained,
“The EPM test shows that he was exposed to the organism in the first test we did which is why we did a follow-up test. Since his exposure level dropped from 1:2000 to 1:1000 this shows that he does not have the disease. There is no good one time test for EPM once they are exposed which is why we had to do the repeat to compare the two.”
While this explanation offered me comfort, I was confused…why does he have any protozoa in his blood if he doesn’t have EPM?
I spoke to another vet and she explained it in a bit more detail…I am hoping I am summarizing what she said correctly..
When a horse tests positive for EPM they either have an active disease or they may not. However, when the test does from 1:2000 down to 1:1000 this typically means that the horse’s immune system is working correctly to fight the disease off- active or not. EPM testing typically provides you with a % of the chance your horse has an active EPM infection, or at least if you send it to Cornell University. For instance, lets say a horse gets the results back and it shows that they are “positive” or have been exposed to S. Neurona (one of the two EPM protozoa)…their results are 1:647. This means that, after doing a bunch of adding and multiplying that this vet kindly did for me, the horse has a 60-70% chance of having ACTIVE EPM. Meaning, he most likely would be symptomatic (ie: behavioral changes, ataxia, weight loss, difficulty eating, changes in soundness, and a bunch of other neurological symptoms).
My hunch is that Chance’s immune system was boosted because I started him on Transfer Factor (amazing stuff… more information can be found in some of my older posts) again as soon as his results came back positive for Lyme.
Here are the 3 EPM tilters that were run on Chance (oldest to most recent) along with his Lyme test results:



An Open Letter To The Horse Of A Lifetime

Equine Podiatry
Medical History
- DDFT Lesion on right hind
- Cervical Spine Arthritis
- Hip discomfort due to past fall
Past Treatments Tried
- Stem Cell Injections: Healed the DDFT lesion in right hind until recently the lesion began to reappear
- Ozone Therapy: Assists in the healing of tissues
- Shock Wave Therapy: Assists in the healing of tissue
- Chriopractic adjustments
- Acupuncture
- Supplements
Initial Consultation
Chance showed decreased movement in his right hip and a audible cracking noise at the suspensory joint. He has edema of both hind fetlocks, Pastern, and Pastern Dermatitis. Chance was unshawed on both hinds due to his inability to stand for long periods of time and his decreased mobility. However, his front adorned clips.
Due to the length of Chance’s front toes and the height of his heels he was unable to evenly distribute his weight (60/40) to his front and hind ends. This would most likely cause increased tension on the DDFT tendons and corresponding ligaments resulting in an increased likelihood of tendon and ligament related injuries. The uneven distribution of weight could also inhibit the horse’s range of motion through his hips resulting in his body compensating for this injury and causing ataxia (balance issues), pain, arthritic changes, and cervical spine misalignment.
By shortening the toe of both front feet, the heel will rise allowing a more even distribution of his weight.
Front


Final Product: Front
Trimmed feet to corrected to the following specifications:
Foot Beginning Angle & Toe Corrected Angles & Toe Total P.C.
L/F 47 Degrees at 3 7/8 inches 53 Degrees at 3 inches 6 Degrees
R/F 45 Degrees at 3 3/4 inches 54 Degrees at 3 inches 9 Degrees
Hind

Final Product: Hind

| Return visit to trim and shoe Chance’s hind feet with #2 OBRHB Wedge shoes.Trimmed hind feet and corrected to the following specifications:
Foot Beginning Angle & Toe Corrected Angles & Toe Total P.C. L/H 48 Degrees at 3 7/8 inches 54 Degrees at 3 1/4 inches 6 Degrees R/H 46 Degrees at 4 1/4 inches 55 Degrees at 3 1/4 inches 9 Degrees Note: Chance needed to be sedated by veterinarian to complete the trim and shoe his hind feet due to preexisting hip and DDFT issues. |

Ozone Therapy
OZONE THERAPY – HISTORY, PHYSIOLOGY, INDICATIONS, RESULTS
Judith M. Shoemaker, DVM 305 Nottingham Road Nottingham, PA 19362
717-529-0526 Fax 717-529-0776
http://www.judithshoemaker.com
Ozone therapy has been utilized and heavily studied for more than a century. Its effects are proven, consistent, safe and without side effects. Why is it not more universal in its use? Many of you have come with some trepidation about infusing a gas into a vessel because you are concerned about emboli, or have some dreadful fear about ozone’s toxicity since we frequently hear about the unhealthy ozone levels in the atmosphere. These fears do not apply to properly administered medical ozone, and the potential benefits of ozone therapy are profound and without associated detrimental effects.
Oxygen, in its several forms, cycles through the atmosphere and life processes just as water does. Ozone is produced in the upper atmosphere when UV light strikes the oxygen rising from plants, plankton, and algae in our forests and seas. It then falls back through the atmosphere, as it is heavier than air, combining with pollutants and water, cleaning the air and forming peroxides that benefit plants. Ultraviolet light breaking down pollutants and nitrous oxides also can produce ozone at the ground level, which is the eye and lung irritant in smog.
Medical ozone, used to disinfect and treat disease, has been around for over 150 years. Used to treat infections, wounds, and multiple diseases, ozone’s effectiveness has been well documented. Ozone has been used to disinfect drinking water since before the turn of the last century. A text on medical ozone therapy was published by Dr. Charles J. Kenworth in 1885! The best technology for producing ozone gas was designed and built by Nikola Tesla in the 1920’s. Heads of leading medical institutions in the U.S. contributed to a 1929 book “Ozone and Its Therapeutic Actions” describing the treatment of 114 diseases using ozone.
In 1933, the AMA began its systematic suppression of all modalities of treatment that did not complement its liaison with the emerging pharmacologic and diagnostic industries. Ozone therapy, along with many other useful therapies, were methodically eliminated from the educational process and exposure to the public in the U.S.
Less suppression has occurred in Europe and other countries, especially in Russia. Today in Germany, and other countries, ozone therapy is commonplace. Over 7000 doctors in Germany use it daily. In fact, in Germany, ozone generators are in ambulances for treatment of stroke victims. The incidence of permanent paralysis in these patients is much less than that in similar patients where ozone is not used.
Ozone generators are relatively simple and inexpensive. The equipment used to handle ozone is readily available but needs to be relatively non-reactive. Glass, Teflon, Kynar, silicon, and gold are completely non-reactive. Equipment made of other substances can contaminate the ozone or just deteriorate rapidly using up the ozone and becoming nonfunctional.
Generators use several technologies to produce ozone
- UV lamp – makes small amounts of ozone and is unreliable in making accurate concentrations. They burn out easily.
- Corona discharge – dual dielectric sealed systems produce ozone but also lots of heat which is both destructive to ozone and to the machine.
- Cold plasma generators – which produce ozone using low level current passed in 2 tubes of a noble gas between which an electrostatic plasma field forms that ionizes the oxygen.Ozone concentration is measured in u/ml or gms/L of oxygen, 5% or 70 u/ml is usually the maximum concentration used in clinical medical applications. High concentrations will damage red cells and inhibit growth of healthy cells.Dosage and frequency protocols vary widely. Initial high dose treatments may “jumpstart” the immune system followed by lower doses. Those who are fearful have been “starting slow and going low” with dosage and still have good results. Concentration must be carefully controlled with accurate flow rates, requiring pediatric regulators for the needed slow flow rates to produce high concentrations. Therefore, home made machines and lesser quality nonmedical devices are not appropriate.
Ozone poteniates free radical scavenging substances and systems in the body, inducing the production of superoxide dismutase, catalase, and glutathione peroxidase. If ozone administration causes any respiratory irritation from out-gassing through the lungs, a bolus dose of 1 to 5 grams of vitamin C can be given and will eliminate any coughing instantly.
Oxygen/ozone mixtures cannot cause emboli when injected at reasonable rates as they dissolve and diffuse very quickly in body fluids, unlike air (predominantly nitrogen) which is what forms emboli and causes the bends or decompression disease.
The physiologic actions of ozone are many, the simplest of which is to provide sufficient oxygen to allow complete oxidation of sugars and other fuels to produce sufficient and efficient energy and to “burn clean” to CO2, water, and inert end products. If not enough oxygen is available, then incomplete oxidation occurs, producing carbon monoxide, lactic acid, and partially oxidized toxins that inhibit further oxygen metabolism and “clog the system”, tying up hemoglobin, water, and the mechanisms for function and elimination.
Administration can be through any route with modifications:
- Direct IV infusion – Ozone slowly administered into a major vessel.
- Major auto-hemotherapy – Anticoagulated blood is mixed with ozone and is infused into a vessel.
- Rectal/vaginal insufflation – Humidified ozone is administered by catheter.
- Minor autohemotherapy – Blood mixed with ozone is injected intramuscularly.
- Limb or body bagging – Body or parts are bathed in humidified ozone.
- Ozonated water – Dissolves easily in water to be used topically or consumed.
- Ozone in Saline or LRS – Can be used topically or given IV or SQ.
- Intra-articular administration – For joint healing and prolotherapy.
- Prolo/Sclerotherapy – Very good, less painful than other agents.
- Acupuncture – With ozone, more effective than B12.
- Ozonated olive oil – Ozone is bubbled through oil until the oil is thickened. This will produce ozonides that are not irritating and thus is applied topically even to eyes.
- Inhalation – Ozone that has been bubbled through olive oil and humidified will not irritate respiratory epithelium.
- Subconjunctival injection – For ulcers and keratitis sicca.
- Gingival and tooth apex injection – Can eliminate infection.
- Urinary bladder insufflation – For chronic inflammation.
- Disc protrusions – Prolotherapy, which can be injected at interspinous space and around facets, stabilize joints and accelerate healing.
- Auricular – Can be direct, humidified, or bagged with a homemade device made from IV bags and tubing (á la Margo Roman).As an anticancer, antiviral, antibacterial, and ant fungal agent, ozone is unsurpassed, especially since there are no appreciable side effects.Oxygen deficit is key to the development and progression of all disease processes. Dr. Otto Warburg’s work, confirmed by others, shows that this deficit and subsequent toxin buildup is the fundamental cause of all degenerative disease, especially cancers.
Antioxidants help the body to protect itself from excessive oxidative damage caused by multiple free radicals, many of which are inactivated by ozone. The support of free radical scavenging systems is important but only oxygen can improve the deficit that makes cells vulnerable to oxidative damage in the first place. Long-term ozone therapy can be augmented by supplementation with antioxidants, but normally they should not be administered within 4 to 12 hours of ozone therapies.
Ozone produces the same effects as exercise, which produces significantly more free radical oxygen than can be administered in any ozone treatment. Ozone equals ”exercise in a syringe” without doing joint damage.
Ozone potentiates more complete oxidation, helps to maintain more normal body temperature and increases the effects of most hormones, vitamins, herbs, homeopathics, and drugs. Concurrent ozone administration reduces the amount of chemotherapeutic drugs needed to achieve effect by 1⁄4 to 3⁄4. It complements chelation therapies and frequently improves the affect and sense of well being in patients.
Continued therapy will allow Herring’s Law to manifest “Healing from inside to outside, top to bottom, front to rear, and in reverse chronological order of the insults to the body.” Healing crises, however, may occur. Ozone therapy facilitates the rapid resolution of these crises.
2005 Judith M. Shoemaker, DVM

Treating Cellulitis in horses
A common and potentially hazardous infection that can be helped with combining antibiotics, cold hosing, and exercise.

On Monday night I showed up at the barn around 7:00 p.m. to ride once the day cooled off. To my dismay I found that Freedom’s knee was hugely swollen. I had wrapped his legs because he’d felt a bit stocked up the night before and because the swelling had no where to go except the knee, the effect was horrifying. Visualize a grapefruit.
Almost immediately I saw the cause: a scrape less than an inch long. Before I called the vet I scrubbed the wound to make sure it wasn’t a puncture wound (didn’t look like it to me, but a puncture would where a joint is involved can be very serious). Normally I would also shave the area around the cut but I had sent my clipper blades out to be sharpened! My guess was cellulitis but since it involved a joint I wanted to makes sure I…
View original post 499 more words

If You Experience Worsening Depression…
Chance began another round of Excede to get his scratches under control- it is a never ending battle. A while back, I had a skin scrape of Chance’s scratches due to their chronic nature. The scrape results showed a number of bacteria, all commonly seen with this type of infection, that were resistant to most antibiotics. Thus why we decided to try Excede.
Administering Excede is pretty straight forward- 1 shot IM every 4 days for about a month. Easy enough….or so I thought. The first shot was administered by the vet when I was not present. The second shot the vet also administered while I was there. Thirty minutes after the shot was given to Chance I noticed he seemed off but not in his “normal” post-acupuncture relaxed state. He suddenly became lethargic, he wouldn’t eat his dinner, and the gut noises became almost nonexistent. I commented to the vet my concerns and she came over and reexamined him. Sure enough something was wrong. She proceeded to administer 10cc of Banamine (just in case it was colic) and told me to walk him around outside for about 20-30 minutes. Then see if he would eat 2 cups of feed only. We walked and Chance began to act like his normal happy go lucky self. Once inside he started to eat!
Part of me felt that his reaction was a fluke. However, the third dose proved me wrong. Four days later, Chance received his shot and went outside to enjoy the first beautiful, warm day. I sat in the field watching him. He was sluggish, lethargic, stiff..he looked 10 years older and barely moved from one spot under a tree. He wasn’t eating grass nor did he run around and play- he didn’t even run up to me like he normally would. I decided to bring him inside and give him a warm bath since it was in the high 70’s. He was non responsive to his bath- no playing with the hose or even accepting peppermints. I placed a cooler on him to ensure he stayed warm until he was out in the sunshine. I figured after a bath he would perk up- again, I was wrong. At dinner time I went to bring him in and typically I will open up the gait and he will canter into his stall- he slowly walked instead. He wouldn’t eat his feed (he normally whinnies and makes a fuss until he gets his feed and devours it) or his hay…I stayed and watched him for a while and he just slept. I spoke to John, the guy who helps me with Chance and Lucky, and he confirmed that Chance hadn’t been finishing his feed and wasn’t running when he brought him in for dinner.
My concerns grew and I decided to do some research on Excede. That strange thing is I usually do extensive research before changing or administering anything with my animals. But, for some reason I did not do so this time and I wish I had.
According to a number of reputable websites, Excede can cause significant and dangerous side-effects such as; diarrhea, severe acid reflux, blood coming from mouth, loss of appetite, lethargy, muscle and gait stiffness, and more.
The most troubling of everything that I read wasn’t what was posted on the Pfizer (the manufacturer) website but from the countless statements given by horse owners and the studies done by outside companies.
According to drugs.com, “in the PK study, several horses developed clinical signs consistent with foot pain (stiff in the front limbs when turned in tight circles, and increased pulses and heat to the front feet). One horse in the NAXCEL group and one horse in the 6.0 mg/lb (2X) EXCEDE group were euthanized due to laminitis. Clinical signs of foot pain (stiff front limbs and increased heat and pulses in feet) affected more horses, for a longer period of time, in all EXCEDE-treated groups as compared to the NAXCEL-treated group. The study housing (multi-horse pens on concrete slabs) and diet (free choice alfalfa/grass mix and once a day pellets) may have contributed to the development of foot pain. The prevalence and severity of injection site reactions in EXCEDE-treated horses may also have contributed to the development of a stiff gait. A causal relationship between ceftiofur and foot pain could not be definitively determined.”
The research has revealed that Excede should be used with caution and the horse receiving the medication must be monitored. Make sure to weigh the benefits and risks before starting Excede. This drug can be lifesaving for many horses but for others, it can be life-threatening.
Excede Resources
Straight from the Horse’s Mouth: Antibiotics, Antifungals, Antivirals
Equine Product Catalog: In depth understanding of equine medications
FINALNewMexicoEIBPetitionExhibits2908-1407_pdf
