Donkeys are known to get a little chunky and by chunky I mean fat deposits externally and internally which are detrimental to their health and wellbeing. Further, keeping your donkey at an ideal weight is of the utmost importance for the prevention of laminitis.
Here is some nutritional information for caring for your donkey:
Feed 1.5-2% of body weight in forage per day.
Generally, once the energy (calorie) requirement has been met, their protein requirement will have also been met. Donkeys also only require about 75% of the calories that a horse of a similar weight would need which is why they are often referred to as “super keepers.”
Donkeys have rather large intestines, which they use to full capacity, and will retain forage longer to digest their intake more thoroughly. Due to their increased capacity and retention, donkeys often have a “hay belly” appearance, or an “A” frame appearance.
1. Feed roughly 75% straw and 25% hay ,except during the winter when you can feed 50/50 straw and hay.
2. Barley straw is ideal, followed by wheat straw and then oat.
3. Vitamin / Mineral supplement or Ration Balancer • Use a low sugar/starch carrier for supplements such as Timothy Pellets or Non-Molasses Beet Pulp. Ration balancing supplements with a 3- to 4-ounce serving size are typically a better choice.
4. Access to water 24/7 despite the belief that they do not need as much water as horses, they DO!
5. Avoid sugary treats.
6. Muzzle. Muzzle. Muzzle. OR Dry Lot. Once your donkey gains weight not only is it difficult to lose, the fat deposits (the fallen crest, lumps) may never go away. It is easier to be proactive than it is to be reactive. Even if the grass looks sparse, due to their “desert” ancestry, any grass is considered “lush.”
Sweet Vera was acting lethargic one evening. She did not show any obvious signs of colic like pawing or distress. However, she was laying down more than typical. Whenever approached she would stand up. The most obvious sign was that when she was offered a treat she was not interested. I took her temperature and it was normal. Gut sounds were present but she looked bloated. I decided to give the vet a call. The vet came and tubed her and gave her some banamine. When Vera was tubed, but due to her small stature, a smaller tube had to be used and not much came out.
The next day she continued to act off. Again, I called the vet and decided to bring her into the hospital. There the vet tubed her at intervals throughout the day and into the next. They gave her fluids via an IV and did a few ultrasounds . Thankfully they were able to get a larger tube in her and the thick, paste like substance started coming out…more and more and more. The interesting part of this was that she does not get grain. There was no sand in the substance that was removed from her belly but my guess is someone gave her treats and due to the extreme heat she was not drinking as much- basically, a perfect storm hit.
Day three she began to perk up, have bowel movements, and even started eating some mash. The next day she was able to return home and has been doing well.
How to Spot Colic in Donkeys?
Dullness
Lying down
Lack of appetite or refusing to eat
Weight shifting, usually between the hind legs
Rolling and pawing at the ground (rare in donkeys, can indicate a serious problem)
Fast breathing, rapid heart rate
Sweating
Brick red or pale gums or insides of eyelids
Dry or tacky gums
Lack of, or reduction in, the normal quantity of droppings
Self-isolating or moving away from companions.
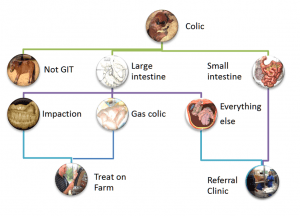
Types of Colic:
Impaction Colic: Impaction occurs when forage, sand, dirt or other material gets lodged in the colon, causing the horse to be unable to pass manure and putting a halt to the whole digestive system. Impaction can also be caused in some cases by enteroliths, naturally occurring mineral deposits that can reach up to 15 pounds in size. Impaction colic tends to occur more in the winter months, due to a lack of hydration.
Gas Colic: Gas colic is a mild, abdominal pain stemming from the result of gas buildup in the horse. This can be caused by a change in diet, low roughage consumption, parasites or administration of wormer.
Sand Colic: Sand colic is caused by the abnormal consumption of large amounts of sand while grazing or eating off dry, sandy ground. Upward of 80 pounds of sand have been found in a colicking horse’s gut. Naturally, sand colic is more common in southern regions where the ground tends to be more mineralized. One way you can help prevent sand colic is to avoid feeding horses from the ground, and instead use a feed pan, bucket or feeder.
Entrapment (or Displacement) Colic: Displacement transpires when the large colon moves to an abnormal location, often occurring at the pelvic flexure, an area where the colon narrows and makes a sharp turn. In some cases, displacement can also lead to entrapment, where something traps the gut and can cut off blood supply.
Enteritis: Abdominal pain can also be caused by enteritis, the general inflammation of the gut. This inflammation is most commonly caused by colonization of the gut by pathogens (bacteria or viruses). Learn more about this in the Importance a Balanced Gut Microbe Ratio in the Gut.
Strangulation (or Gut Torsion or Twisting) Colic: A twist occurring in the gut causes strangulation colic, which often cuts off blood supply and results in dying tissue. This type of colic is very serious and the most likely to be fatal.
Enterolith: Enteroliths are mineral accumulations of magnesium-ammonium-phosphate (struvite) around a foreign object (a piece of metal, pebble, bailing twine, hair, rubber) that form round, triangular, or flat stones inside the bowel usually over the course of multiple years. They form in the large colon of horses where they can remain for some time until they move and cause an obstruction in the large or small colon, resulting in colic.
Idiopathic or Spasmodic Colic: The majority of colic cases are idiopathic. This means the cause is unknown or unable to be determined. This is a wide-ranging term for horses presenting with colic where other abnormalities cannot be found, and, which generally have increased gut movement (and therefore gut noise if you listen over the belly). The colic signs are associated with increased gut spasm due to the increase in motility (a horse equivalent to gut cramps that we may experience after a very spicy curry for example). Rectal examination is within normal limits in these cases and, these horses often respond very favorably to drugs that decrease gut motility (see treatment of colic).
Treatment Options:
Your vet may carry out the following to try to diagnose the type of colic:
Checking your donkey’s heart rate and temperature.
Listening to your donkey’s abdomen with a stethoscope to check the gut sounds
Checking your donkey’s teeth
Taking a blood sample
Performing a rectal examination
Passing a stomach (nasogastric) tube to check for reflux (backed up food or fluid). Your vet will decide on the best treatment based on your donkey’s diagnosis and are likely to give painkillers.
Depending on their findings, your vet may give your donkey fluids via a nasogastric tube or put them on a ‘drip’ (usually via the large vein in their neck). It may take multiple visits from your vet to treat your donkeys colic.
Your donkey may need to be hospitalised if their case is severe. If your donkey is hospitalised, their companion must go too, as hospitalisation can be very stressful for donkeys. Some types of colic need surgery to resolve them, which will require prompt transport to a hospital. Surgery carries a high risk in most colic cases and involves considerable nursing care and cost. Check you are insured for the costs and talk to your vet about the chances of success.
Euthanasia may be the kindest option if your donkey’s case is serious.
Prevention:
Colic is so dangerous because by the time your donkey lets you know it has colic, it may be too late to save it. The old adage, ‘prevention is better than cure’, definitely applies.
Observe your donkey daily, looking for any changes in behaviour. Know what typical dung looks like. Be aware of the average number of piles of droppings your donkeys pass each day and the consistency. Persistently very loose or very dry droppings could be indicative of colic, particularly if other symptoms appear. Check your donkey’s breathing pattern so you will be able to spot any change.
Colic Causes & Prevention:
Feed – sudden changes to diet, poor quality feed, too much grass, feeding cereals:
Make any dietary changes gradually over at least a week, ideally 2-4 weeks
Feed good quality forage and donkey specific proprietary feeds
Avoid moldy feed
Always soak sugar beet to the manufacturer’s recommendations
Feed little and often, especially if your donkey has additional feed
Do not allow your donkey access to too much rich spring grass.
Inadequate or dirty water supply:
Check troughs daily. Self-filling drinkers can become blocked, or the water supply can fail
Clean dirty water containers as donkeys will not drink dirty water
Check water is not frozen or too cold. Many donkeys will not drink very cold water
Offer several sources of water.
Eating non-food items such as plastic bags, rope or bedding:
Ensure your donkeys cannot access non-food items
Change your donkey’s bedding to something less palatable, such as wood shavings
Do not use cardboard or paper bedding.
Eating poisonous plants:
Know your poisonous plants and trees
Remove poisonous plants or fence off the problem area
Check pasture, boundary fences and hedgerows frequently
Fence off trees when fruiting to prevent your donkey gorging.
Sandy soil:
Avoid grazing on sandy soil pasture if possible.
Dental disease – failure to chew food adequately resulting in a blockage of the gut:
Have your donkey’s teeth checked at least annually by a qualified equine dental technician or vet
Dental disease is more common in older donkeys
Suspect dental problems if donkeys are ‘quidding’ (dropping part chewed feed) or drooling saliva
Parasites – worms causing obstruction or inflammation of the gut:
Arrange regular faecal worm egg counts to check if your donkey needs treating for worms
Speak to your vet for advice
Clear droppings from your donkey’s paddock at least twice a week.
Stomach ulcers:
Keep stress to a minimum
Trickle feed your donkey.
Pain – any painful condition can lead to colic, including severe lameness:
Ensure your donkey has adequate pain relief if they have a painful condition.
So, I wish I did not have to start this process again…but unfortunately, I do. Once again I have a senior horse with a variety of acute and chronic conditions that all hit at the same time. Right now I am trying to make her comfortable while also trying to figure out what is what and how to best respond.
Three months ago Tilly was tested for EPM due to muscle wasting and weight loss.The first time she was in the lower end of an active infection. We started a compounded medicine for 1 month and her numbers decreased. We decided to do another round as she responded well to the first round. However, the numbers remained the same. We also tested her for Lyme which showed a chronic and an active infection but the numbers were in the high normal range and the vet felt that it was not treatment worthy at the time.
Last month Tilly began “crab walking” out of the blue. Called the vet. They came out. Her ataxia was bilateral- both her left and right hind- whereas EPM tends to be unilateral. Further, her presentation was not suggestive of Lyme.
We started steroids (dexamethasone oral power) for 5 days with Banamine, tapering as we went, and she seemed to recover. The consensus was it was an acute attack that may have occurred given she is a senior with a history of being an Amish workhorse and perhaps, she pulled something in her neck.
Treatment was complete and another week went by and again, she showed some ataxia. This time less severe. The vet felt that since she responded well to the first round of steroids that it was not EPM-related as you would not see improvement. Further, if it were Lyme related the presentation would be more consistent. Again, a round of Dex and improved quickly. The next week we had her neck x-rayed and there were some arthritic changes. However, she was running around and moving well so the vet felt injections in her neck would not be necessary at that time.
Seventy two hours later, she had some trouble getting up but eventually succeeded. The next morning my sweet girl was spinning, crab walking, and falling over. It was absolutely terrible to see. I immediately gave her 10cc IV Banamine and she calmed down and stopped spinning. The vet came out and administered Dex IV and thought that due to her inflammatory bowel disease we should try Dex IM to ensure absorption. We also decided to pull blood to test for Cushings as she seemed to lose weight overnight and was not shedding out well. The next day she was lame on her right front. Panicked I called the vet fearing that if she did have Cushings, she was trying to founder due to the steroid use. Thankfully, the vet came out, did a nerve block on her right front (this helps to see if the horse has laminitis as they will improve once blocked) and checked for pulses (if a horse has laminitis typically they will have pulses in their hooves) and Tilly did not have any. So, the vet did not feel we were dealing with founder. However, the lameness presented a major challenge due to her still being ataxic on the hind end. The vet did cortisone injections into her neck hoping to help with inflammation due to arthritis. Tilly did great and suddenly, began freaking out. Spinning, knocking into the doors, etc. The vet explained that the injections likely added more pressure on her spinal cord causing her to react. Again, once the vet was able to safely administer Banamine and some Dorm, she calmed and laid down for the first time in over a week for a good 45 minutes. We decided to make sure she was able to get back up. Although she had some trouble, after a couple tries, she was able to do so. Her breathing was heavy, wheezy, almost like she was having a panic attack and hyperventilating. A few minutes later, her breathing returned to normal.
Tilly’s Cushing’s text level was about 100 pg/mL (it should be about 30 pg/mL during mid-November to mid-July) meaning, she does have Cushings. The vet decided to wean her off of the steroid as to not increase the risk of Laminitis even more but also to give neck injections time to work (5-7 days). We also immediately began Prescend (2 tabs) a day to treat her Cushings.
We are on day 5 since the 3rd ataxic episode and day 3 post neck injection and she is still lame on her right front along with ataxic on her hind end. However, she is still eating, engaging, and is bright and alert. She does not seemed distressed or in pain thankfully. Due to Tilly not showing much improvement (even though it can take 5-7 days to see improvements from the neck injections) I decided to start her on a non-compounded EPM medication, Protazil. According to the vet, Protazil should not cause any harm whether her symptoms are EMP related or not. I also began 10cc of Vitamin E oil. Tilly was previously on pelleted Vitamin E but due to her inflammatory bowel disorder, she may struggle to absorb the pelleted form of the supplement. Further, there are a number of studies showing the benefits of Vitamin E and the connection between Vitamin E and ataxia.
On a positive note, since starting Prescend for her Cushings, I have noticed that she is drinking less water. Increased water intake is a symptom of unmanaged Cushings. I am hopeful that means the medication has started to work at regulating her hormones. We are now at a wait and see point. I continue to try to make her comfortable. Tons of bedding in her huge foaling stall, hay everywhere, fans on, doors open. She has been a trooper. My hope is that she recovers from this and enjoy whatever time she has left and fights this as she has so many other things- the reason she was given the name, Ottilie.
The most common esophageal conditions in horses is choking and it is always an emergency.
Typically, there is a cause to this condition like eating too quickly, food being too dry or suck together, or even a lack of water. Some horses may choke due to their dental health as well. Further, abnormal esophagus anatomy can also contribute a predisposition to choking, Food may form a firm bolus that becomes lodged in their esophagus. However, other items can also cause an obstruction like hay or straw, hard treats, carrots, and even, nonfood objects.
How to tell if your horse is choking?
The most common symptoms are hyper salivation, food or foam coming out of their nose and mouth
Some horses may become anxious and thrash around
Retching
Not eating
Acting colicky
Coughing
What to do when you suspect your horse is choking?
Immediately remove access to any food or hay.
Call your veterinarian
If you are knowledgable with medication administration, and your horse is extremely agitated, you can administer a non-steroidal anti-inflammatory (NSAID) like Banamine. Make sure to check the horse’s temperature before administering as NSAIDs will mask a fever.
Once the vet arrives they will preform a physical exam. Typically, they will insert a tube down the horse’s throat to flush out any compaction. This may have to be done multiple times.
Your horse maybe required to begin antibiotics depending on the veterinarian’s advise to help treat any aspiration or potential pneumonia.
You may need to keep your horse confined for a few horses (or days) depending on the severity of the choke.
You will need to check their temperature for a few days after choke to ensure that the horse has not developed an upper respiratory infection.
Depending on the cause, the veterinarian may schedule a dental float procedure, or have you wet the horse’s feed and/or hay or switch the feed entirely.
My senior Belgian Draft mare has a chronic condition where her stools are relatively solid but after having a stool, she passes fecal liquid separately, Her tail and hind end, and legs are covered. Initially when she came to me she had loose stools and the vet did a fecal and we put her on Biosponge. Her Fecal Sample showed minimal infestation and the Biosponge did not do much. Over time, her stools became more solid but the liquid continued. Now, after being with me for about 6 months we are still having this issue.
So, I did some research and came across an article on something I had never heard of before- Fecal Water Syndrome. According to an article on SmartPak.com, Fecal Water Syndrome is typically caused by the following;
The underlying cause of FWS in horses is not known at this time and there are many theories as to why some horses develop it. A group of researchers in Germany set out to explore some of the proposed theories and discovered that neither dental disease nor a heavy parasite burden seemed to be associated with FWS. However, it was found to be more likely to occur:
in horses of low rank or “pecking order” in the social hierarchy of a herd
in winter when subordinate horses were confined to a smaller space, leading to anxiety
in geldings vs mares, which are usually more dominant than geldings
in paint horses
However, the article also noted that due to FWS being a relatively new diagnosis, more studies are needed to look at the role stress, nutrition, and potentially, other factors in the development and management of FWS.
Diagnosis of FWS
Most veterinarians approach the diagnosis of a horse with FWS similar to one with diarrhea or loose stool. That is, they start by taking a thorough history from the owner, then perform a complete physical examination with special emphasis on the digestive system, and finally may recommend specific tests to evaluate the health of the horse in general and the GI tract in particular. It can be helpful to confirm the presence of soiled hind limbs and tail as well as dirty stall walls and bedding. While on the farm, the vet may want to walk through the regular feeding and management programs including turnout and herd status.
Treatment and Management of FWS
Although there is no standard treatment or set of recommendations for the care and feeding of horse suffering from FWS, all potential causes for disruption in the GI system should be addressed, including social stress.
Making adjustments to the horse’s turn-out time and group.
Making adjustments to the diet (with the input of a veterinarian and nutritionist.)
Trying out various medications and supplements one at a time on the passage of fecal water. For example, adding omega 3 fatty acids for a normal inflammatory response in the gut, and to the stabilizing effects of “baker’s yeast” or Saccharomyces cerevisiae.
Make sure to keep the hindquarters clean and dry to prevent any sores for forming.
Tilly came to me from a slaughter auction in Texas after 17-ish years as an Amish workhorse. She was thin (she still is), sick (upper respiratory infection) had cracked hooves, had never had her teeth floated (they made a horrible grinding and clicking sound when she ate), and apparently had never been clipped or bathed or worn a blanket. I do not think she had ever even had a treat (she still won’t take an apple or carrot).
SYMPTOMS:
Rumbling gut
Cow pie stools
Grinding/clicking teeth
Cracked hooves
Dull coat
Underweight
Running nose
PROFESSIONALS:
Farrier for evaluation and trimming
Dentist for power float of teeth
Vet for physical, blood work, and fecal
TESTING/RESULTS:
CBC: all in normal range aside from her creatinine and protein suggesting dehydration. These values normalized after about 1 week)
Fecal: Minimal
FEED:
Triple Crown Senior Feed (Low sugars, low starch, high fat)
Tons of water with Horse Quencher added
Salt block
MEDICATIONS:
Exceed injections (2 total a week apart) then SMZ for 2 weeks
Banamine
Brewer’s Yeast (Stomach)
BioSponge (Gut health and to tackle her loose stools)
Due to Draft horses being prone to certain diseases such as, metabolic ailments like PSSM (Polysaccharide storage myopathy), laminitis, Cushings, founder, tying-up, and shivers diet is imperative. Based on these ailments, starch and sugar calories should be replaced by fiber and fat calories.
It is recommended that these guys have high quality forage and some concentrates while working due to their slower metabolism (similar to ponies). Meaning that the less energy they use, the more weight they gain. High carbohydrate feed should be avoided, as a forage with a rational balancer and/or a low NSC feed.
Breakdown of How To Feed A Draft Horse
Calorie Breakdown:
15% daily calories from sugar
20-25% daily calories from, fat
No less than 1% of horse’s body weight in forage
Calculating Fat Content:
Pounds of feed per day x % of fat
For example,
3 lbs of feed= 3 x 0.25= 0.75 lb fat
Feed Brands:
Feeds should have no more than 33% sugar and starch (low carb).
Low in starch and sugars: soy, beat pulp, wheat bran, wheat middlings
Feeds with 20%+ of fat should be supplemented with rice bran (20% fat). Feed with anything less than 20% should be supplemented with 100% additional fat source.
Nutrena Compete
Purina Strategy
Blue Seal Hunter, Demand, Vintage Gold
Southern States Legend
Supplements:
Oil: soy oil, canola, corn oil, rice bran
Vitamin E & Selenium supplement (be careful when adding in selenium as high levels can be toxic)
The Plan
Either Purina Strategy or Southern States Legend: No more than 5-6 lbs of feed per 1000 lbs
Rice Bran Oil: begin with 1/4 cup and increase by 1/4 cup every few days until 2 cups are reached. Continue with 3-4 cups per day.
Vitamin E with Selenium: 1-2 oz per day
Forage: Alfalfa pellets mixed or substituted with Purina or Southern States feed
Mix 12 parts alfalfa (or Purina or Southern States Feed or mix of the two) with 1 part water. Soak for 10 minutes. Add in oil. Let it sit for 2+ hours. Right before feeding add in the supplement (Vet E/Selenium).
Few horse owners are aware of this disease which is a progressive, paralyzing disease that is 80-100% fatal in affected horses. Botulism is sometimes referred to as “forage poisoning” in adult horses or “shaker foal syndrome” in foals. The disease is caused by a potent toxin that is produced by the bacterium Clostridium botulinum. This bacterium lives in the soil as well as the intestinal tract of many normal birds and mammals, including the horse. It produces dormant spores that can be found in 18.5% of soil samples tested in the United States. The disease is most prevalent in Kentucky, Ohio, Maryland, Pennsylvania, California, and Tennessee although it can occur in any state in the U.S. Clostridium botulinum produces several different toxins. Type A toxins are often implicated in human infant botulism and are most often found west of the Rocky Mountains. Types B, C, and D toxins are usually involved in cases of equine botulism, with Type B responsible for 85% of horse cases in the U.S.
Horses of any age are susceptible to botulism which may be initiated by one of three ways. In the case of “forage poisoning” the horse ingests toxins that are contaminating feedstuffs such as grain or hay. Feed contamination is most often due to putrefied carcasses of birds or rodents. A Type C botulism outbreak that killed a number of horses in California several years ago was traced back to hay that contained the infected carcass of a rabbit. The bacteria can also enter a horse’s body via contamination of a wound, especially a deep puncture wound. A good example is “Shaker foal syndrome” which is most frequently caused by the bacteria entering the newborn foal’s body through the foal’s moist navel. Something that can be minimized by dipping the foal’s navel in mild iodine solution soon after birth. The third method in which the disease can be initiated is by ingestion of the spores in the soil. The ingested spores activate in the horse’s intestinal tract where they produce potent toxins that are then absorbed. Regardless of the route, once the bacteria have entered the horse’s body they produce toxins that block transmission of nerve impulses to the horse’s muscles. This results in a progressive paralysis of all the major muscle groups and is concluded with paralysis of the diaphragm, which results in death. Once symptoms develop, death may ensue in several hours or take up to a week.
The disease is difficult to diagnose because it resembles several other medical conditions and diseases such as choke, colic, rabies, EPM, and sleeping sickness. Blood samples very rarely contain toxin and necropsy following the death of the horse usually does not provide a conclusive diagnosis. Because the bacteria often occur naturally in the horse’s intestinal tract, isolation of the organism from the sick horse’s intestine is not diagnostic.
Clinical signs of the disease in adult horses suffering from “forage poisoning” initially include loss of facial expression, a sleepy appearance, saliva drooling from the corner of the mouth, loss of tongue control and loss of tail tone. The horse’s appetite is good, but it has a great deal of difficulty in chewing food and appears to be “playing” in their feed and water buckets. As muscular weakness becomes more profound, the horse will experience muscle trembling, generalized sweating and labored breathing. A weakened, shuffling gait may develop and the horse may take stiff, short steps as if walking on eggs. Eventually, the horse goes down and death results due to paralysis of the respiratory muscles. “Shaker foal syndrome” is usually seen in foals one to two months of age but can develop as early as two weeks or as late as 8 months of age. Early signs in foals are similar to those seen in adults in that the foal shows generalized weakness, poor tail tone, and loss of tongue control. The foal will often dribble milk from the mouth and nostrils because of an inability to swallow. Because of muscle weakness, the foal will lie down frequently. When it does rise, it soon develops muscle tremors and collapses. Affected foals may die within 12 hours of exhibiting symptoms or may linger for as long as a week.
Botulism is usually fatal if left untreated. Prior to the advent of antitoxin, the death rate among affected foals was greater than 90%. With the use of antitoxins in conjunction with antibiotics and supportive therapy, the mortality rate can be reduced to less than 25%. Animals unable to swallow should be fed through a nasogastric tube and placed on IV fluids. Once the toxin produced by the bacteria is attached to the nerve ending it cannot be neutralized by the antitoxin. Therefore, early treatment is critical. Even with aggressive therapy, recovery is slow and may require up to two weeks before the affected horse recovers.
Because of the high death rate and the difficulty in diagnosing this disease, prevention through vaccination is critical. A Type-B Toxoid vaccine is available and is quite effective in preventing the disease. In areas where the disease is prevalent, pregnant mares should be initially vaccinated at the 8th, 9th and 10th month of gestation and thereafter at the 10th month of each pregnancy. Yearly vaccination of adults in areas where the disease frequently occurs is also recommended. If unable to vaccinate the mare prior to foaling, limited information suggests that foals vaccinated with the toxoid at 2 weeks, 4 weeks and at 8 weeks of age developed adequate protection, even in the presence of passive maternal antibodies. Currently, no licensed vaccines are available for preventing botulism due to Cl. botulinum types A or C or other subtypes of toxins. Cross-protection between subtypes does not occur.
As in all horse health issues, your local veterinarian is your best source of information.
ABOUT THE AUTHOR:Thomas R. Lenz, DVM, M.S., Diplomate of the American College of Theriogenologists, is a trustee of the American Horse Council, past chairman of AQHA’s research committee and past president of the American Association of Equine Practitioners. This article is provided courtesy of AAEP Alliance Partner, AQHA.
I have been desperately trying to get my miniature donkey, Lucky, to drop some lbs. The thing with Lucky- he literally gained weight overnight. One day he was a skinny mini and the next he had a potbelly. I was really concerned that the weight suddenly appeared and had the vet run a heptic panel to ensure he wasn’t experiencing some sort of liver dysfunction. Sort of like how humans can develop Ascites when they have liver related disease. Anyways, his blood work came back and all was okay….he was just fat!
Unlike horses, donkeys develop “fat deposits” around their neck, abdomen, and butt and even once the weight has been lost the deposits stay for life!
The Dangers of Obesity in Donkeys
According to the Scarsdale Vets;
“Obesity increases the risk of developing hyperlipaemia and laminitis, both of which can be fatal. Prevention of obesity is better than cure, because rapid loss of condition in overweight donkeys can trigger hyperlipaemia.
Hyperlipaemia is a condition in which triglycerides (fats) are released into the circulation which can result in organ failure and death unless treated rapidly. The early signs of dullness and reduced appetite can be difficult to detect. Hyperlipaemia can be triggered by anything that causes a reduction in food intake e.g. stress, transport, dental disease.
Laminitis is a condition in which there is inflammation in the laminae of the foot that connect the pedal bone to the hoof wall. This can progress to rotation or sinking of the pedal bone within the foot. The cause is not fully understood and many factors are involved but obese animals are more prone to develop the disease.”
Equine Metabolic Syndrome: “Overweight donkeys often develop a fat, crest neck and fat pads around their tail base. When this occurs the donkey can develop a metabolic disease known as ‘Equine Metabolic Syndrome’. This causes insulin resistance and increased levels of blood glucose (blood sugar) in the blood stream. In equids this can lead to recurrent episodes of laminitis or founder. This disease involves inflammation of the white lining or laminar junctions of the feet, extreme foot pain and difficulty walking. In severe cases this can also cause changes in the bone of the foot and hoof wall” (Yarra Ranges Animal Clinic)
How To Help Your Donkey Lose Weight Safely
Use a muzzle
Limit grazing
Ask your vet to do blood work to ensure your donkey is healthy
Have the dentist come out and examine the donkey’s teeth
For the past 6 weeks, my horse has been receiving Ozonetherapy to aid in his chronic back leg related issues- dermatitis (“scratches”), previous DDFT tendon laceration, a history of Lymphingitis, and the residual scar tissue from his DDFT injury. Due to his age (27), he lacks proper circulation in his hind end which does not help him fight his pastern dermatitis.
According to the American Academy of Ozonetherapy, Ozonetherapy is described as;
“Ozonotherapy is the use of medical grade ozone, a highly reactive form of pure oxygen, to create a curative response in the body. The body has the potential to renew and regenerate itself. When it becomes sick it is because this potential has been blocked. The reactive properties of ozone stimulate the body to remove many of these impediments thus allowing the body to do what it does best – heal itself.”
“Ozonotherapy has been and continues to be used in European clinics and hospitals for over fifty years. It was even used here in the United States in a limited capacity in the early part of the 20th century. There are professional medical ozonotherapy societies in over ten countries worldwide. Recently, the International Scientific Committee on Ozonotherapy (ISCO3) was formed to help establish standardized scientific principles for ozonotherapy. The president of the AAO, Frank Shallenberger, MD is a founding member of the ISCO3.”
“Ozonotherapy was introduced into the United States in the early 80’s, and has been increasingly used in recent decades. It has been found useful in various diseases;
It activates the immune system in infectious diseases.
It improves the cellular utilization of oxygen that reduces ischemia in cardiovascular diseases, and in many of the infirmities of aging.
It causes the release of growth factors that stimulate damaged joints and degenerative discs to regenerate.
It can dramatically reduce or even eliminate many cases of chronic pain through its action on pain receptors.
Published papers have demonstrated its healing effects on interstitial cystitis, chronic hepatitis, herpes infections, dental infections, diabetes, and macular degeneration.”
After doing research and speaking to one of my good friends, we determined that Chance’s flare up of Lymphingitis, after almost 3 years of not a single issue, could possibly be caused by his immune system’s response to Ozonetherapy. Let me explain.
Chance suffers from persistent Pastern dermatitis (“scratches”) since I purchased him in 2000. I have tried everything- antibiotics, every cream and ointment and spray for scratches, diaper rash ointment, iodine and vaseline mix, Swat, laser treatments, scrubs and shampoos, shaving the area, wrapping the area, light therapy…you name it, I have tried it. So, when we began Ozonetherapy to help break down the left over scar tissue from his old DDFT injury, I noticed that his scratches were drying up and falling off. We continued administering the Ozonetherapy once a week for about 6 weeks. The improvement was dramatic!
However, one day Chance woke up with severe swelling in his left hind leg and obviously, he had difficulty walking. He received Prevacox and was stall bound for 24 hours. The vet was called and she arranged to come out the following day. The next morning, Chance’s left leg was still huge and he was having trouble putting weight on it. I did the typical leg treatments- icing, wrapping. The swelling remained. I tried to get him out of his stall to cold hose his leg and give him a bath but he would not budge. He was sweaty and breathing heavily and intermittently shivering. So, I gave him an alcohol and water sponge bath and continued to ice his back legs. I sat with him for 4 hours waiting for the vet to arrive. He had a fever and wasn’t interested in eating and his gut sounds were not as audible. He was drinking, going to the bathroom, and engaging with me. I debated giving him Banamine but did not want it to mask anything when the vet did arrive.
The vet arrived, gave him a shot of Banamine and an antihistamine and confirmed that Chance had a fever of 102 degrees and had Lymphingitis. There was no visible abrasion, puncture, or lump… I asked the vet to do x-rays to ensure that he did not have a break in his leg. The x-rays confirmed that there was no break. The vet suggested a regiment of antibiotics, steroids (I really am against using steroids due to the short-term and long-term side effects but in this case, I would try anything to make sure he was comfortable) , prevacox, and a antacid to protect Chance from stomach related issues from the medications. It was also advised to continue to cold hose or ice and keep his legs wrapped and Chance stall bound.
The following day, Chance’s legs were still swollen but his fever had broken. The vet called to say that the CBC had come back and that his WBC was about 14,00o. She suggested that we stop the steroids and do the antibiotic 2x a day and add in Banamine. I asked her if she could order Baytril (a strong antibiotic that Chance has responded well to in the past) just in case. And that is what we did.
Being as Chance had such a strong reaction to whatever it was, I did some thinking, discussing, and researching…first and foremost, why did Chance have such an extreme flare up of Lymphingitis when he was the healthiest he has ever been? And especially since he had not had a flare up in 3+ years…plus, his scratches were getting better not worse. The Ozonetherapy boosted his immune system and should provide him with a stronger defense against bacteria, virus’, etc. So why exactly was he having a flare up? And that is when it hit me!
In the past when Chance began his regiment of Transfer Factor (an all natural immune booster), he broke out in hives. The vet had come out and she felt it was due to the Transfer Factor causing his immune system to become “too strong” and so it began fighting without there being anything to fight, thus the hives. My theory- Chance started the Ozonetherapy and his body began to fight off the scratches by boosting his immune system. As the treatments continued, his immune system began to attack the scratches tenfold. This resulted in his Lymphatic system to respond, his WBC to increase, and his body temperature to spike. Makes sense…but what can I do to ensure this is not going to happen again?
My friend suggested attacking the antibiotic resistant bacteria by out smarting them…okay, that seems simple enough…we researched the optimal enviroments for the 3 types of bacteria present where Chance’s scratches are (shown in the results of a past skin scape test). The bacteria – E. Coli, pseudomonas aeruginosa and providencia Rettgeri. The literature stated that PA was commonly found in individuals with diabetes…diabetes…SUGAR! How much sugar was in Chance’s feed? I looked and Nutrina Safe Choice Senior feed is low in sugar…so that is not it. What else can we find out? The optimal temperature for all three bacteria is around 37 degrees celsius (or 98.6 degrees fahrenheit), with a pH of 7.0, and a wet environment. Okay, so, a pH of 7.0 is a neutral. Which means if the external enviroment (the hind legs)pH is thrown off, either to an acidic or alkaline pH, the bacteria will not have the optimal enviroment to continue growing and multiplying. How can I change the pH?
Vinegar! An antimicrobial and a 5% acetic acid! And…vinegar is shown to help kill mycobacteria such as drug-resistant tuberculosis and an effective way to clean produce; it is considered the fastest, safest, and more effective than the use of antibacterial soap. Legend even says that in France during the Black Plague, four thieves were able to rob the homes of those sick with the plague and not become infected. They were said to have purchased a potion made of garlic soaked in vinegar which protected them. Variants of the recipe, now called “Four Thieves Vinegar” has continued to be passed down and used for hundreds of years (Hunter, R., 1894).
I went to the store, purchased distilled vinegar and a spray bottle and headed to the farm. I cleaned his scratches and sprayed the infected areas with vinegar. I am excited to see whether our hypothesis is correct or not…I will keep you posted!