https://www.theodysseyonline.com/an-open-letter-to-the-horse-of-lifetime?ref=fb


Resources on how to diagnose, treat, prevent, and handle lameness in horses
Your Horse Has a Swollen Leg – Why and What To Do | EquiMed – Horse Health Matters
Fetlock Lameness – It’s importance… | The Horse Magazine – Australia’s Leading Equestrian Magazine
Causes of Equine Lameness | EquiMed – Horse Health Matters
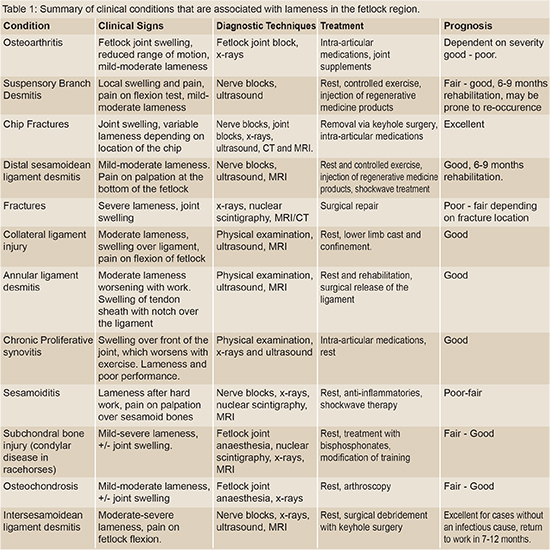
Common Causes of Lameness in the Fetlock

Medical History
Past Treatments Tried
Initial Consultation
Chance showed decreased movement in his right hip and a audible cracking noise at the suspensory joint. He has edema of both hind fetlocks, Pastern, and Pastern Dermatitis. Chance was unshawed on both hinds due to his inability to stand for long periods of time and his decreased mobility. However, his front adorned clips.
Due to the length of Chance’s front toes and the height of his heels he was unable to evenly distribute his weight (60/40) to his front and hind ends. This would most likely cause increased tension on the DDFT tendons and corresponding ligaments resulting in an increased likelihood of tendon and ligament related injuries. The uneven distribution of weight could also inhibit the horse’s range of motion through his hips resulting in his body compensating for this injury and causing ataxia (balance issues), pain, arthritic changes, and cervical spine misalignment.
By shortening the toe of both front feet, the heel will rise allowing a more even distribution of his weight.
Front


Final Product: Front
Trimmed feet to corrected to the following specifications:
Foot Beginning Angle & Toe Corrected Angles & Toe Total P.C.
L/F 47 Degrees at 3 7/8 inches 53 Degrees at 3 inches 6 Degrees
R/F 45 Degrees at 3 3/4 inches 54 Degrees at 3 inches 9 Degrees
Hind

Final Product: Hind

| Return visit to trim and shoe Chance’s hind feet with #2 OBRHB Wedge shoes.Trimmed hind feet and corrected to the following specifications:
Foot Beginning Angle & Toe Corrected Angles & Toe Total P.C. L/H 48 Degrees at 3 7/8 inches 54 Degrees at 3 1/4 inches 6 Degrees R/H 46 Degrees at 4 1/4 inches 55 Degrees at 3 1/4 inches 9 Degrees Note: Chance needed to be sedated by veterinarian to complete the trim and shoe his hind feet due to preexisting hip and DDFT issues. |

Judith M. Shoemaker, DVM 305 Nottingham Road Nottingham, PA 19362
717-529-0526 Fax 717-529-0776
http://www.judithshoemaker.com
Ozone therapy has been utilized and heavily studied for more than a century. Its effects are proven, consistent, safe and without side effects. Why is it not more universal in its use? Many of you have come with some trepidation about infusing a gas into a vessel because you are concerned about emboli, or have some dreadful fear about ozone’s toxicity since we frequently hear about the unhealthy ozone levels in the atmosphere. These fears do not apply to properly administered medical ozone, and the potential benefits of ozone therapy are profound and without associated detrimental effects.
Oxygen, in its several forms, cycles through the atmosphere and life processes just as water does. Ozone is produced in the upper atmosphere when UV light strikes the oxygen rising from plants, plankton, and algae in our forests and seas. It then falls back through the atmosphere, as it is heavier than air, combining with pollutants and water, cleaning the air and forming peroxides that benefit plants. Ultraviolet light breaking down pollutants and nitrous oxides also can produce ozone at the ground level, which is the eye and lung irritant in smog.
Medical ozone, used to disinfect and treat disease, has been around for over 150 years. Used to treat infections, wounds, and multiple diseases, ozone’s effectiveness has been well documented. Ozone has been used to disinfect drinking water since before the turn of the last century. A text on medical ozone therapy was published by Dr. Charles J. Kenworth in 1885! The best technology for producing ozone gas was designed and built by Nikola Tesla in the 1920’s. Heads of leading medical institutions in the U.S. contributed to a 1929 book “Ozone and Its Therapeutic Actions” describing the treatment of 114 diseases using ozone.
In 1933, the AMA began its systematic suppression of all modalities of treatment that did not complement its liaison with the emerging pharmacologic and diagnostic industries. Ozone therapy, along with many other useful therapies, were methodically eliminated from the educational process and exposure to the public in the U.S.
Less suppression has occurred in Europe and other countries, especially in Russia. Today in Germany, and other countries, ozone therapy is commonplace. Over 7000 doctors in Germany use it daily. In fact, in Germany, ozone generators are in ambulances for treatment of stroke victims. The incidence of permanent paralysis in these patients is much less than that in similar patients where ozone is not used.
Ozone generators are relatively simple and inexpensive. The equipment used to handle ozone is readily available but needs to be relatively non-reactive. Glass, Teflon, Kynar, silicon, and gold are completely non-reactive. Equipment made of other substances can contaminate the ozone or just deteriorate rapidly using up the ozone and becoming nonfunctional.
Generators use several technologies to produce ozone
Ozone poteniates free radical scavenging substances and systems in the body, inducing the production of superoxide dismutase, catalase, and glutathione peroxidase. If ozone administration causes any respiratory irritation from out-gassing through the lungs, a bolus dose of 1 to 5 grams of vitamin C can be given and will eliminate any coughing instantly.
Oxygen/ozone mixtures cannot cause emboli when injected at reasonable rates as they dissolve and diffuse very quickly in body fluids, unlike air (predominantly nitrogen) which is what forms emboli and causes the bends or decompression disease.
The physiologic actions of ozone are many, the simplest of which is to provide sufficient oxygen to allow complete oxidation of sugars and other fuels to produce sufficient and efficient energy and to “burn clean” to CO2, water, and inert end products. If not enough oxygen is available, then incomplete oxidation occurs, producing carbon monoxide, lactic acid, and partially oxidized toxins that inhibit further oxygen metabolism and “clog the system”, tying up hemoglobin, water, and the mechanisms for function and elimination.
Administration can be through any route with modifications:
Antioxidants help the body to protect itself from excessive oxidative damage caused by multiple free radicals, many of which are inactivated by ozone. The support of free radical scavenging systems is important but only oxygen can improve the deficit that makes cells vulnerable to oxidative damage in the first place. Long-term ozone therapy can be augmented by supplementation with antioxidants, but normally they should not be administered within 4 to 12 hours of ozone therapies.
Ozone produces the same effects as exercise, which produces significantly more free radical oxygen than can be administered in any ozone treatment. Ozone equals ”exercise in a syringe” without doing joint damage.
Ozone potentiates more complete oxidation, helps to maintain more normal body temperature and increases the effects of most hormones, vitamins, herbs, homeopathics, and drugs. Concurrent ozone administration reduces the amount of chemotherapeutic drugs needed to achieve effect by 1⁄4 to 3⁄4. It complements chelation therapies and frequently improves the affect and sense of well being in patients.
Continued therapy will allow Herring’s Law to manifest “Healing from inside to outside, top to bottom, front to rear, and in reverse chronological order of the insults to the body.” Healing crises, however, may occur. Ozone therapy facilitates the rapid resolution of these crises.
2005 Judith M. Shoemaker, DVM


A common and potentially hazardous infection that can be helped with combining antibiotics, cold hosing, and exercise.

On Monday night I showed up at the barn around 7:00 p.m. to ride once the day cooled off. To my dismay I found that Freedom’s knee was hugely swollen. I had wrapped his legs because he’d felt a bit stocked up the night before and because the swelling had no where to go except the knee, the effect was horrifying. Visualize a grapefruit.
Almost immediately I saw the cause: a scrape less than an inch long. Before I called the vet I scrubbed the wound to make sure it wasn’t a puncture wound (didn’t look like it to me, but a puncture would where a joint is involved can be very serious). Normally I would also shave the area around the cut but I had sent my clipper blades out to be sharpened! My guess was cellulitis but since it involved a joint I wanted to makes sure I…
View original post 499 more words

Chance began another round of Excede to get his scratches under control- it is a never ending battle. A while back, I had a skin scrape of Chance’s scratches due to their chronic nature. The scrape results showed a number of bacteria, all commonly seen with this type of infection, that were resistant to most antibiotics. Thus why we decided to try Excede.
Administering Excede is pretty straight forward- 1 shot IM every 4 days for about a month. Easy enough….or so I thought. The first shot was administered by the vet when I was not present. The second shot the vet also administered while I was there. Thirty minutes after the shot was given to Chance I noticed he seemed off but not in his “normal” post-acupuncture relaxed state. He suddenly became lethargic, he wouldn’t eat his dinner, and the gut noises became almost nonexistent. I commented to the vet my concerns and she came over and reexamined him. Sure enough something was wrong. She proceeded to administer 10cc of Banamine (just in case it was colic) and told me to walk him around outside for about 20-30 minutes. Then see if he would eat 2 cups of feed only. We walked and Chance began to act like his normal happy go lucky self. Once inside he started to eat!
Part of me felt that his reaction was a fluke. However, the third dose proved me wrong. Four days later, Chance received his shot and went outside to enjoy the first beautiful, warm day. I sat in the field watching him. He was sluggish, lethargic, stiff..he looked 10 years older and barely moved from one spot under a tree. He wasn’t eating grass nor did he run around and play- he didn’t even run up to me like he normally would. I decided to bring him inside and give him a warm bath since it was in the high 70’s. He was non responsive to his bath- no playing with the hose or even accepting peppermints. I placed a cooler on him to ensure he stayed warm until he was out in the sunshine. I figured after a bath he would perk up- again, I was wrong. At dinner time I went to bring him in and typically I will open up the gait and he will canter into his stall- he slowly walked instead. He wouldn’t eat his feed (he normally whinnies and makes a fuss until he gets his feed and devours it) or his hay…I stayed and watched him for a while and he just slept. I spoke to John, the guy who helps me with Chance and Lucky, and he confirmed that Chance hadn’t been finishing his feed and wasn’t running when he brought him in for dinner.
My concerns grew and I decided to do some research on Excede. That strange thing is I usually do extensive research before changing or administering anything with my animals. But, for some reason I did not do so this time and I wish I had.
According to a number of reputable websites, Excede can cause significant and dangerous side-effects such as; diarrhea, severe acid reflux, blood coming from mouth, loss of appetite, lethargy, muscle and gait stiffness, and more.
The most troubling of everything that I read wasn’t what was posted on the Pfizer (the manufacturer) website but from the countless statements given by horse owners and the studies done by outside companies.
According to drugs.com, “in the PK study, several horses developed clinical signs consistent with foot pain (stiff in the front limbs when turned in tight circles, and increased pulses and heat to the front feet). One horse in the NAXCEL group and one horse in the 6.0 mg/lb (2X) EXCEDE group were euthanized due to laminitis. Clinical signs of foot pain (stiff front limbs and increased heat and pulses in feet) affected more horses, for a longer period of time, in all EXCEDE-treated groups as compared to the NAXCEL-treated group. The study housing (multi-horse pens on concrete slabs) and diet (free choice alfalfa/grass mix and once a day pellets) may have contributed to the development of foot pain. The prevalence and severity of injection site reactions in EXCEDE-treated horses may also have contributed to the development of a stiff gait. A causal relationship between ceftiofur and foot pain could not be definitively determined.”
The research has revealed that Excede should be used with caution and the horse receiving the medication must be monitored. Make sure to weigh the benefits and risks before starting Excede. This drug can be lifesaving for many horses but for others, it can be life-threatening.
Excede Resources
Straight from the Horse’s Mouth: Antibiotics, Antifungals, Antivirals
Equine Product Catalog: In depth understanding of equine medications
FINALNewMexicoEIBPetitionExhibits2908-1407_pdf

My old guy has always had issues with his cervical spine/neck. Throughout the years he has developed arthritis which has caused symptoms which mirror EPM such as; ataxia, difficulty bending, hind end weakness, difficulty going up hills, lethargy, difficulty balancing when foot is lifted, muscle atrophy, sore back…you get the picture.
When his symptoms first came on I had the vet test for EPM. The test was positive. I did my research and found out that about 50% of horses will test positive for EPM but only 1% show actual impairment from the virus. I went ahead and completed two rounds of EPM medication therapy and still his symptoms continued. So, I sought out another vet who practiced eastern and western medicine.
After some chiropractic adjustments and acupuncture she felt that his issues were actually due to the cervical spine and not EPM. The vet also showed me how, when looking at Chance straight on, one of his eyes was lower then the other- a classic sign of cervical and jaw issues. We continued with the chiropractic and acupuncture therapy and have continued for over a year and the change has been remarkable. Along with these therapies, we upped his feed, added supplements, began stretches and different exercises, and had him walking and running up and down hills whenever he was outside. The dentist has also been of great help by floating Chance’s teeth every few months instead of once a year. This helps with the alignment of his teeth because he tends to ware one side of his teeth down more then the other; ultimately straining his jaw and neck.
He has rebuilt the muscle on his hind end, put on around 100 lbs, and is able to do stretches while someone is holding his foot up. He runs when he is outside and is no longer on pain medications (except on the rare occasion).
Here is some useful information on a horse’s back and cervical spine.
Diagnosing A Horse’s Neck Problems
Main Causes of Ataxia in Horses

What type of shoe should I use on Chance’s back feet?
I am looking for something that is glue-on, provides support and comfort, that has good grip, while providing protection for his hoof from the rocky terrain.
After some research, I found GluShus- a company out of England. Their shoes sound fantastic. They have an aluminum shoe set in rubber that glues onto the hoof. Read more about these shoes by clicking the link below.
I’ll let you know how it goes!

Over the last couple weeks the rain has been unrelenting. And with rain comes scratches (Pastern Dermatitis). In a previous entry I spoke about an amazing treatment for scratches that actually worked…however, when it rains like it has recently, once again the scratches got out of control.
A handful of months ago I got a skin scrape on Chance’s hind legs to determine the bacteria that was causing the scratches. Sure enough there were three types of bacteria growing which was why I was having so much difficulty getting them under control.
Below are the results:

As you can see above, the bacteria shows resistance or no interpretation to all but 7 antibiotics. I spoke to my vet and she suggested beginning with Gentamicin and go from there if he does not respond to the medication. Chance has been receiving an injection of 30 mls of Gentamicin in his muscle once a day for about a week now. He obviously does not enjoy this, nor do I for that matter, but his scratches are showing improvements! He is also on the topical cream, Silver Sulfadiazine, once a day.
Fingers crossed that I will get ahead of the scratches and they will go away forever!
The other day I noticed that Chance’s back fetlock a were slightly swollen and he was visably stiffer then normal. I also noticed a golf ball sized lump in the middle of the his chest. It wasn’t super sensitive and looked like a tick bite reaction, except there was no tick and a tiny barely noticeable scratch.
I put a Poltace wrap on his back right leg (which was the leg he had previously injured and received stem cell injections in) and gave him some pain medication. I also started him on Baytril and Ulcerguard as a precaution as previously advised by the vet.
I made an appointment with our vet to come ultrasound his hind right leg and she was to come out in the next two days. I was incredibly anxious to say the least.
The vet arrived and explained that the lump on Chance’s chest was a hematoma from another horse biting him or from him hitting something. Nothing to worry about, it was just the pooling of fluids to lowest point.
I then trotted Chance back and forth as the vet watched. After an exam and the ultrasound, the vet explained that she felt that the swelling was due to Chance’s hip pain and the Pastern dermatitis that we have been treating and we’re finally coming off.
The ultrasound showed a tiny DDFT lesion (vet referred to as a defect that shouldn’t be causing any symptoms). The ultrasound also showed scar tissue that we need to get “stretched out” so that he can gain increased flexibility and work as a protection for Chance’s tendons and legiments. The ultrasound also showed some fluid build up as well. Chance’s Fetlock looks good as do his legiments.
The vet wants Chance to stay on Baytril and Ulcerguard until complete. She also has added a 5 day course of Benadryl and steroids to help with edema of back hind legs.
She also provided me with a shampoo that is milder to clean off scratches and apply swat after cleaning. The vet explained that she didn’t understand why people picked the scabs from the scratches because they’re super deep and pulling the scabs off does more harm than good.
The Vet commented on Chance’s weight gain and how great his skin looks gooded. She wants me to continue working on the scratches and continue doing physical therapy on hills to build up his hind end then get farrier out for back feet.
All and all I feel good about how Chance is doing and feeling. He is still full of energy, eats like he hasn’t eaten in a week, and his eyes and coat are bright. He is not on daily pain medication and is only given it when he is not feeling great. Aside from a few hiccups, Chance is loving life and being spoiled!

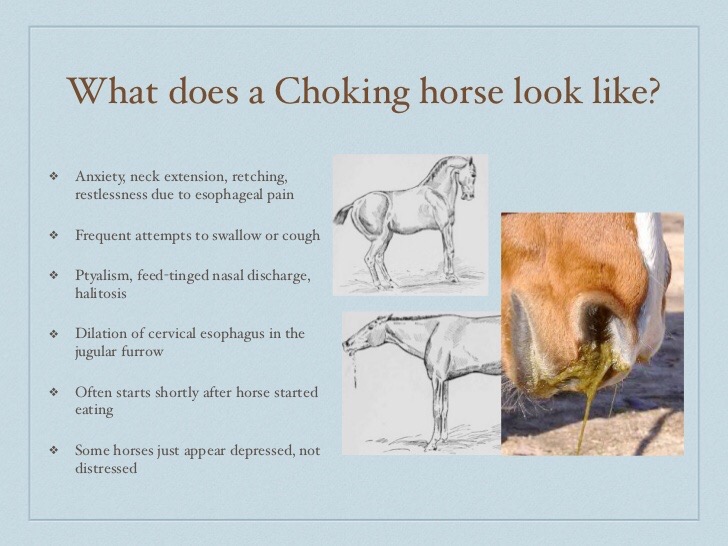
What do you do when your horse suddenly chokes?!
Well, unfortunately, I found out the hard way. Thankfully I had my emergency medical barn book and was able to quickly reference what to do.
Here are the steps an owner can take until the vet comes (if necessary):
1. Help keep your horse calm
2. Give injection Intramuscularly (IM) or Intravenously (IV) or orally (liquid only) of Banamine (10cc) to help relax the muscles
3. Rub the horse’s throat until the substance the horse is choking on comes out of the nose and mouth
4. Remove all other feed and hay
5. Call vet to ask if the horse should be put on antibiotics in case they have aspirated (the substance getting into their lungs)
Here is a link to more information on what you and/or your vet can do to help your horse- When a horse chokes
A handful of months ago I decided to get my horse, Chance, a companion. He has always loved miniature horses but we already had one at the farm (with a very strong personality) so I decided on a miniature donkey. That is when I found Lucky.
Well, Chance did NOT like Lucky from the moment he saw me leading Luck off the trailer. Chance paced and neighed incessantly until he actually broke into a sweat!
I have tried everything- putting them in neighboring stalls, putting them in neighboring paddocks, walking one outside while the other one is grazing, putting something of Lucky’s near Chance’s stall so he could get familiar with the smell, etc.
Today Lucky decided to escape out of his stall and run out to where Chance was. At first Chance just stared, then he went after Luck but he stopped once Luck moved a few feet away. Slowly, Luck inched his way closer and closer until he was a handful of feet away from where Chance was grazing. Chance didn’t seem to even care.
Fingers crossed this is the beginning of a forced, we-will-put-up-with-each-other friendship.



Looking a lot better after almost a years worth of treatments and trying to gain weight!

Standing on all fours!

The muscle atrophy is slowly but surely disappearing and being replaced by muscle.

Sadie watching the horses in the field.
By: Christy Corp-Minamiji, DVM
Any discussion of therapeutic shoeing in the horse must begin with a discussion of what therapeutic shoeing is–and what it is not. According to Stephen O’Grady, DVM, MRCVS, professional farrier and owner of Northern Virginia Equine, in Marshall, therapeutic shoeing (or therapeutic farriery) is “the science and art of affecting/influencing the structures of the foot.” It is not a cookie-cutter, “apply shoe A to foot B” magic bullet in the war on equine lameness. To understand how the foot structures can be influenced, we should first have a clear picture of those structures and the forces that act on them.
“In an ideal world, you would begin from a diagnosis,” says Andrew Parks, MA, VetMB, MRCVS, Dipl. ACVS, professor of Large Animal Medicine at the University of Georgia’s College of Veterinary Medicine. “From that diagnosis you would get your treatment goals. By goals I mean the big picture concepts for treatment. You need to have principles (a range of techniques) that allow you to implement your goals.”
O’Grady concurs: “In order to be proficient at therapeutic farriery you must understand the forces that affect the foot. Excess forces or stresses on the hoof capsule lead to deformation, and excess forces or stresses on the internal structures of the foot lead to disease. Everything we are trying to do with therapeutic farriery is to change the forces on the foot.”
For Want of a Foot …
“There is no definition of a perfect foot,” says Parks. What’s considered a “normal” equine foot differs among breeds and disciplines. Thus, when evaluating trimming and shoeing options for a horse, owners and farriers must first consider foot conformation–what you see when you look at a horse standing at rest. Also evaluate limb conformation, which can affect how the horse’s foot bears weight and the way a horse wears a hoof or a shoe. Both limb and hoof conformation might alter the horse’s stride and landing, affecting the forces upon the foot structures. For instance, a club-footed horse’s high-set heels will alter weight distribution, placing more pressure on the toe and heel. While farriery might alter the distribution of the load on the foot, one misconception that O’Grady would like to correct is the idea that you can “change limb conformation by trimming. After 6-8 months (of age), conformation is conformation,” he says. Rather than attempting to make an atypically conformed foot or leg appear “normal,” O’Grady stresses the importance of trimming “for the cards the horse has been dealt.”

Figure 1: This illustration shows the forces around the center of rotation (the black dot) in a horse at rest. The ground reaction force is transmitted upward through the lamellae to the bony column. The extending force of the coffin joint is balanced by an equal flexing force generated by the deep digital flexor tendon.
The Foundation: An Appropriate Trim
According to O’Grady, therapeutic shoeing must begin with an appropriately trimmed foot. While much is made of hoof “balance,” O’Grady dislikes the term as he feels it is not clearly defined among practitioners and farriers. He prefers to work from a set of landmarks as clear guidelines to trim each individual foot appropriately:
1) Pick up the foot, and draw a line across the widest part of it. This line will fall just in front of the center of rotation (at the coffin joint). A well-trimmed foot should have approximately even proportions of hoof on either side of that line.
2) Look at the frog. The heels should lie approximately on the same line as the widest part of the frog.
3) Stand the horse on a hard, flat surface so his cannon bone on the leg you’re addressing is perpendicular to the ground. A line drawn down the front of the pastern should be parallel to a line drawn along the dorsal (toe) surface of the hoof wall. This is the hoof-pastern-axis (HPA). A broken-back HPA, in which the front of the foot is angled less steeply than the pastern, shows up in low heels; a broken-forward axis manifests in high heels (club foot).
According to O’Grady, anyone can use these three parameters to assess a horse’s trim. “Trimming is the mainstay of therapeutic shoeing,” he states. Thus, any benefit to be derived from therapeutic shoeing must have a basis in an appropriately trimmed foot. “The first function of a shoe is to protect that which is trimmed and also to complement it,” he says. “Then you can add mechanics … to that trim.”
Physics and the Equine Foot
Newton’s Third Law of Motion states that for every action there is an equal and opposite reaction. Similarly, the support and movement of the equine foot depends upon a system of opposing forces. Understanding these forces is key to understanding the principles of farriery.
In the standing horse:
1) The ground reaction force (GRF, as pictured in Figure 1) is the force transmitted from the ground to the ground surface of the foot, into the hoof wall, and from the wall through the lamellae (interlocking leaflike tissues attaching the hoof to the coffin bone) to the bony column.1 Think of the GRF as the ground pushing up as the foot lands. The GRF extends (i.e., an extensor motion rather than flexor) the coffin and pastern joints and is centered at the center of rotation.2 The GRF is counteracted by two forces.
2) The first of these forces, the weight of the horse, is transmitted down the cannon bone through the fetlock. Since the GRF and the weight of the horse through the cannon bone are both vertical but not aligned, they cause the pastern to rotate so the fetlock becomes closer to the ground.
3) At rest, the horse’s anatomy counters this effect by the upward and backward force of the deep digital flexor tendon (DDFT)–the flexing force illustrated in Figure 1. Picture a string attached to the back of the coffin bone and pulled upward over the navicular bone, over the fetlock, and along the back of the cannon toward the knee.




{kind=link}